, Jiyoung Min, MS1, Jiwon Shinn, BA1, Oak-Kee Hong, PhD3, Jang-Won Son, MD, PhD4, Seong-Su Lee, MD, PhD4, Sung-Rae Kim, MD, PhD4, Soon Jib Yoo, MD, PhD4
, Jiyoung Min, MS1, Jiwon Shinn, BA1, Oak-Kee Hong, PhD3, Jang-Won Son, MD, PhD4, Seong-Su Lee, MD, PhD4, Sung-Rae Kim, MD, PhD4, Soon Jib Yoo, MD, PhD4 
1Department of Medical Informatics, College of Medicine, The Catholic University of Korea, Seoul, Korea
2Division of Endocrinology and Metabolism, Department of Internal Medicine, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
3Department of Internal Medicine, College of Medicine, The Catholic University of Korea, Seoul, Korea
4Division of Endocrinology and Metabolism, Department of Internal Medicine, Bucheon St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Bucheon, Korea
Copyright © 2021. Korean Society of Cardiovascular Disease Prevention; Korean Society of Cardiovascular Pharmacotherapy.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Funding
This work was supported by a National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIT) (No. 2020R1A2C1003464).
Conflict of Interest
The authors have no financial conflicts of interest.
Author Contributions
Conceptualization: Kim HS, Yoo SJ; Data curation: Kim HS, Min J, Shinn J, Hong OK, Son JW, Lee SS, Kim SR, Yoo SJ; Formal analysis: Kim HS, Min J, Hong OK, Son JW, Lee SS, Kim SR, Yoo SJ; Methodology: Kim HS, Son JW, Lee SS, Kim SR, Yoo SJ; Supervision: Yoo SJ; Writing - original draft: Kim HS, Yoo SJ; Writing - review & editing: Yoo SJ.


Categorical variables were reported as frequencies (%), and continuous variables were reported as mean±standard deviation.
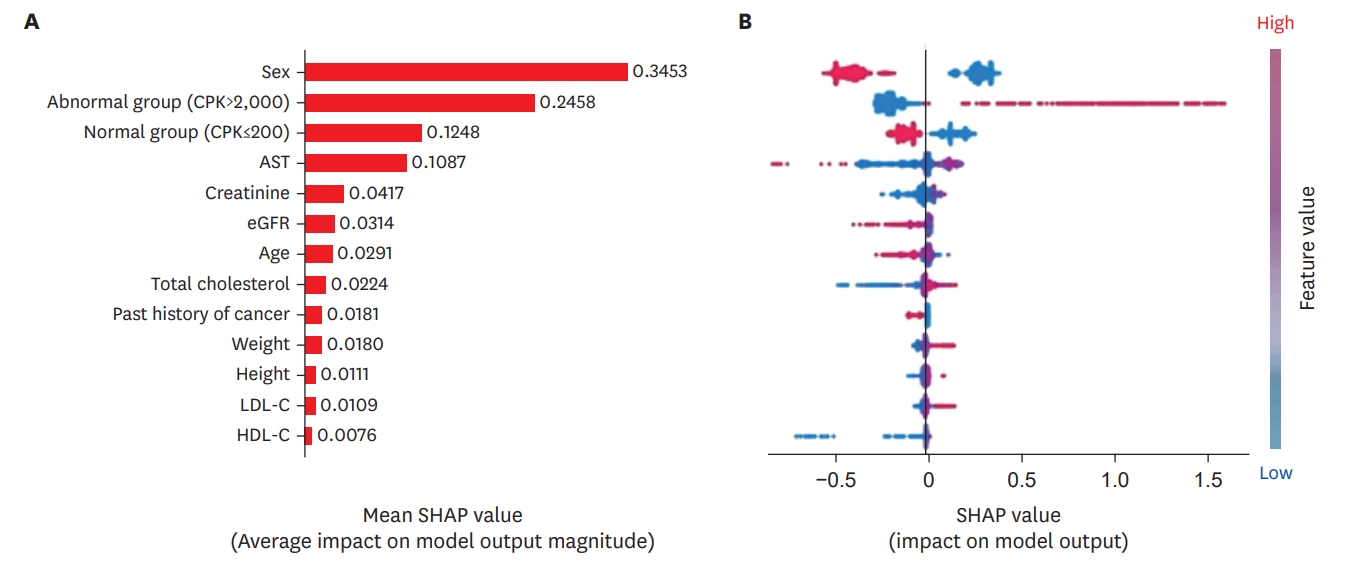
ALT = alanine aminotransferase; AST = aspartate aminotransferase; BUN = blood urea nitrogen; CK = creatine kinase; eGFR = estimated glomerular filtration rate; HDL-C = high-density lipoprotein cholesterol; LDL-C = lowdensity lipoprotein cholesterol.

 PubReader
PubReader ePub Link
ePub Link Cite
Cite