ABSTRACT
- Obesity reduces life expectancy, lowers quality of life, and causes numerous cardiometabolic diseases and some cancers. However, the individual risk of developing obesity-associated comorbidities is highly variable and cannot be explained only by body mass index. Observations that some obese people have a low risk for cardiometabolic disorders gave rise to the notion of metabolically healthy obesity (MHO). Despite the lack of a precise definition, MHO is typically identified by normal glucose and lipid metabolism indices, as well as the absence of hypertension. In individuals with MHO, the absence of metabolic abnormalities may minimize the risk of mortality, cardiovascular diseases, chronic kidney disease, dementia, and cancer, compared to metabolically unhealthy individuals with obesity. However, MHO appears to be a temporary phenotype that may not confer permanent benefits to individuals with obesity, further justifying therapeutic efforts to maintain metabolic fitness. In this review, we describe the traits of the MHO phenotype, its changeable nature, and the factors associated with phenotype change. In addition, we discuss the clinical outcomes of the MHO phenotype, particularly focusing on the transition of metabolic health over time and its effect on cardiometabolic disorders. Finally, the clinical importance of maintaining metabolic health is emphasized.
-
Keywords: Metabolic syndrome; Obesity; Weight reduction; Weight gain
INTRODUCTION
- Obesity is a complex, multifactorial chronic disease associated with a higher risk of comorbidities such as metabolic syndrome, cardiovascular disease (CVD), and several types of cancer, as well as a higher risk of death from those comorbidities [1,2]. Obesity has a significant impact on patients’ quality of life, limits economic and social activity, and imposes a significant financial burden on society as a whole. Despite several efforts to address the obesity pandemic and its consequences, obesity remains a serious public health concern globally [1,2]. The Korean Society for the Study of Obesity (KSSO) defines obesity as a body mass index (BMI) ≥25 kg/m2 according to the Asia-Pacific criteria of the World Health Organization guidelines, which is different from that used in Western countries [3,4]. According to the 2020 Obesity Fact Sheet by KSSO using the Korean definition, the prevalence of overall obesity was 32.6% in 2009 and increased by 1.18-fold to 38.5% in 2018, respectively [5]. Therefore, obesity is clearly a major public health problem in Korea and across the world.
- However, not all obese people are at an elevated risk of obesity-related comorbidities and mortality, implying that there is a subset of healthy obese people, who have a condition known as "metabolically healthy obesity (MHO)” [6–10]. Metabolic abnormalities, such as dyslipidemia, insulin resistance, hypertension, and an unfavorable inflammatory profile, are absent in MHO [7–10]. Numerous studies have demonstrated that people with MHO have a lower risk of mortality and other comorbidities than those with metabolically unhealthy obesity (MUO) and are not at a higher risk than people who are normal weight [7–10]. However, so far, the predictive value of the MHO phenotype, as well as its clinical definition and criteria, remains a subject of debate [11,12]. Furthermore, the clinical implications of the MHO phenotype may be dependent on the health outcomes being studied [12]. Furthermore, as evidence mounts that MHO is changeable across time, researchers’ focus has shifted to the consequences of phenotypic shifts in MHO individuals. In this context, the purpose of the present review was to address numerous contemporary issues concerning MHO, such as its natural course and clinical consequences, with a special emphasis on its dynamic and variable nature.
DYNAMIC AND CHANGEABLE ASPECTS OF MHO
- Obesity has been considered to be a chronic and easily relapsing disease [13–15]; these traits of obesity also apply to MHO. Individuals in long-term obesity treatment programs may experience cycles of weight reduction and weight return, with their phenotypic shifting from MUO to MHO and back again. Furthermore, nearly half of the MHO participants in the Multi-Ethnic Study of Atherosclerosis (MESA) acquired metabolic abnormalities by the end of the 12-year follow-up period [16]. This conclusion is corroborated by a meta-analysis based on estimates from 40 studies, which showed that MHO individuals had higher risk of progressing to the abnormal metabolic state than their counterparts with metabolically healthy nonobesity (MHNO), and half of the MHO individuals would lose their metabolic health over time [17]. Similarly, in a 6-year follow-up study of the prospective Pizarra trial, 30% of people classified with MHO at baseline transitioned to MUO [18]. Using the Korean National Health Insurance Service-National Health Screening Cohort (NHIS-HEALS), our study team demonstrated the transitional character of the MHO phenotype [19]. Only 57.2% of the initial MHO group in the Korean cohort remained metabolically healthy after 2 years, whereas 42.8% experienced aggravation in their metabolic health—in other words, transition to MUO status. However, MUO also showed a transient and reversible nature, as 11.8% of the baseline MUO group restored their metabolic health (i.e., transitioned from MUO to MHO) [19]. Therefore, the shift from MHO to MUO is not always a one-way street. Finally, as the phenotypic transition frequently occurs in both MHO and MUO, we need to focus on the implications of these transitions in health outcomes in obese patients.
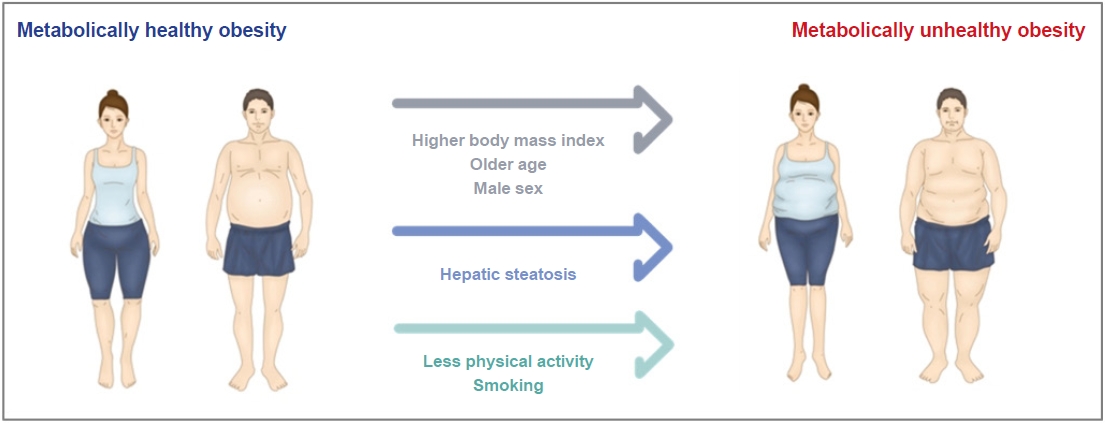
- High BMI, older age, evidence of more severe metabolic dysfunction (i.e., the presence of hepatic steatosis, number of abnormal metabolic criteria, and values closer to the upper limit of the normal range), and a poor lifestyle index (a composite of diet composition, leisure time physical activity, and cigarette smoking) all increase the risk of transitioning from MHO to MUO (Fig. 1) [16,20–24]. The North West Adelaide Health Study (NWAHS) of 4,056 randomly selected adults revealed that maintenance of an MHO phenotype, which was associated with favorable outcomes, was related to younger age and a more peripheral fat distribution [25]. Female sex, younger age, and lower initial weight and BMI were found to be significant predictors of sustained metabolic health in a primary care cohort from the Clinical Practice Research Datalink in the United Kingdom [22]. Our cohort study on the MHO phenotype and its CV outcomes also showed that a higher BMI and the presence of any risk factor at baseline were associated with a higher likelihood of incident impaired metabolic state [19].
CLINICAL OUTCOMES OF MHO WITH CONSIDERATION OF ITS DYNAMIC CHANGES
- CV outcomes and mortality
- The notion of MHO was derived from evidence indicating that a subgroup of obese adults lacks relevant cardiometabolic risk factors, hence reducing their risk of CVD [20,26,27]. Despite this notion, numerous studies have revealed detrimental long-term effects in MHO populations [27–29]. Indeed, previous research showed that patients with MHO had a higher risk of CVD than MHNO individuals [28]. Using a Korean nationwide population-based cohort, our research team discovered that MHO status was associated with a significant risk of CV events, showing that MHO is not a benign condition in terms of CVD [19]. The risk of CV events was greater in the MHO group than in the MHNO group (hazard ratio [HR], 1.14; 95% confidence interval [CI], 1.05–1.24). In an updated analysis of metabolic health status and BMI 2 years after the baseline examination, we further discovered that the cardiovascular outcomes of the MHO group varied substantially according to their status change over time. Among participants with MHO initially, those who transitioned to MUO had a higher risk of CV events than those who maintained MHO status (HR, 1.24; 95% CI, 1.00–1.54). Several cohort studies found poor CV outcomes in individuals who moved from MHO to a metabolically unhealthy phenotype [16,30,31]. In accordance with these prior studies, our findings demonstrated that MHO at baseline does not ensure a favorable CV outcome for patients, especially when the switch to a metabolically unhealthy phenotype occurs.
- The term "obesity paradox" was adopted to explain the observation that, although higher BMI is associated with higher rates of diabetes, hypertension, dyslipidemia, and CVD, obese individuals with these conditions may have better survival outcomes than leaner individuals [32,33]. Similarly, those classed as normal weight or underweight may have a worse prognosis for CVD than those who are overweight, a phenomenon known as the "lean paradox" [34]. Our research indicated that, despite the higher incidence of cardiovascular events in obese people regardless of their metabolic health, their all-cause mortality was comparable to or lower than that of nonobese, healthy people [19]. Indeed, MHO status at baseline was related to lower mortality than MHNO (HR, 0.86; 95% CI, 0.79–0.93) [19]. Those who transitioned from the MHO to the metabolically unhealthy nonobesity (MUNO) group—that is, shifting to a metabolically unhealthy status while concurrently losing body weight—had a higher all-cause mortality rate than those who remained in the MHO status (HR, 1.96; 95% CI, 1.45–2.65). These data provide support for the "lean paradox" and highlight the heterogeneous nature of the MHO population. Interestingly, the shift from MUO to MUNO was also associated with significantly increased all-cause mortality (HR, 1.31; 95% CI, 1.15–1.49) when the persistent MUO group was used as the reference, but the transition from MUO to MHO was associated with lower all-cause mortality (HR, 0.77; 95% CI, 0.64–0.93). These findings further reinforce the "lean paradox" by demonstrating that a catabolic condition, as indicated by weight loss, may be a powerful predictor of a poor prognosis. Further research on therapeutic interventions to prevent progression to a metabolically unhealthy phenotype might aid in improving the health effects of obesity.
- Diabetes
- Diabetes is a major public health issue causing several comorbidities and mortality worldwide, with an increasing incidence and prevalence [35]. According to the International Diabetes Federation Diabetes Atlas, 537 million adults aged 20 to 79 years had diabetes in 2021, and this number is expected to climb to 783 million by 2045 [36]. The reasons for the diabetes epidemic are numerous, including an increased prevalence of obesity-related to a sedentary lifestyle and unhealthy diet [37].
- Large-scale epidemiological studies conducted in Europeans, Japanese, and Koreans found that MHO adults had a significantly higher risk of developing type 2 diabetes (T2D) than the respective MHNO reference groups [12,25,38,39]. The risk of developing T2D is substantially lower in those with MHO than in those with MUO, but it is still approximately fourfold higher than in those with MHNO [38] and is strongly related to the number of metabolic abnormalities [40–42]. In a 6-year follow-up cohort study of a rural Chinese population, the participants with baseline MHO had an elevated risk of T2D, with an adjusted HR of 1.94 (95% CI, 1.33–2.81) [43]. However, the risk of T2D was higher for people who experienced the transition from MHO to MUO when compared to stable MHNO, but not for participants who did not experience this transition [43]. As a result, maintaining a metabolically healthy status is clinically important to alleviate the risk of incident diabetes in patients with obesity.
- Chronic kidney disease
- Obesity is an established risk factor for chronic kidney disease (CKD) [44–46]. To date, few longitudinal studies have investigated the risk of developing CKD in individuals with MHO [45,47–49]. In 2015, a Japanese study group reported that the MHO phenotype was not associated with a higher risk of developing CKD [49]. On the contrary, more recent studies have consistently proposed a significant association between MHO phenotype and incident CKD [45,47,50]. For example, a prospective cohort study including 62,249 metabolically healthy, young, and middle-aged men and women without CKD or proteinuria at baseline, showed that overweight and obesity were associated with an increased incidence of CKD [47]. Our research group investigated CKD risk in individuals with the MHO phenotype, with consideration of its phenotypic transition over time [51]. Based on initial health examination results, MHO status was associated with an elevated incidence of CKD (HR, 1.23; 95% CI, 1.12–1.36), suggesting that MHO is not a benign condition in the context of renal outcomes. In a follow-up analysis of metabolic health status and BMI, we found that the risk of incident CKD in the MHO group was highly variable according to the phenotypic transition. The risk of incident CKD was particularly high in people who had progressed to a metabolically unhealthy phenotype (i.e., MHO to MUNO or MUO) compared with the stable MHNO group (MHO to MUNO group: HR, 1.60; 95% CI, 1.16–2.20; MHO to MUO group: HR, 1.68; 95% CI, 1.45–1.96). In contrast, people who reduced their body weight and maintained metabolic health were not at a higher risk for developing CKD than the stable MHNO group (MHO to MHNO group: HR, 0.98; 95% CI, 0.72–1.32). These data suggest that although people with MHO are at a high risk of CKD development, the risk of developing CKD could be mitigated if their body weight is well controlled while maintaining metabolic health. In other words, our results have important clinical implications that obesity is a modifiable risk factor in preventing CKD development in people with MHO, as well as emphasizing the significance of metabolic health in CKD development.
- Colorectal cancer
- Obesity is also related to the incidence of certain forms of cancer [52]. Obesity, in particular, is a risk factor for colorectal cancer (CRC), one of the most frequent gastrointestinal malignant tumors globally [53]. To date, investigations have yielded contradictory results about the risk of CRC in MHO patients; nevertheless, an elevated risk of CRC has been found to be strongly related to MUO [54–58]. As a result, it is uncertain whether obesity, independent of obesity-related metabolic abnormalities, plays a role in the development of CRC. We investigated the relationship between obesity, metabolic health, and the transition of metabolic phenotype with CRC risk. The study comprised 319,397 patients from the Korean nationwide health examination cohort, and we divided obese patients into four groups based on their dynamic metabolic health status: MHO, MHO to MUO, MUO to MHO, and stable MUO [59]. We observed no significant difference in incident CRC risk in the stable MHO group, compared to the stable MHNO group (HR, 0.97; 95% CI, 0.83–1.14). The MHO to MUO group, in contrast, had a higher incidence of incident CRC than the stable MHNO group (HR, 1.34; 95% CI, 1.15–1.57). Among patients with MUO at baseline, those who transitioned to the MHO group had no elevated risk of CRC (HR, 1.06; 95% CI, 0.91–1.25), but those who stayed in the stable MUO group had a higher risk of incident CRC than those who moved to the stable MHNO group (HR, 1.29; 95% CI, 1.19–1.41). Therefore, we suggest that when assessing the relationship between obesity and CRC, physicians should examine patients' metabolic health conditions and counsel them on the necessity of metabolic fitness.
- Dementia
- Obesity, as previously noted, is a well-known risk factor for a variety of cardiometabolic disorders and some types of cancer. However, obesity has been found to be protective against dementia in recent studies [60–64]. Recently, two cohort studies evaluated the effects of obesity without metabolic abnormalities on Alzheimer's disease (AD) incidence [65,66]. A Korean study employing a nationwide cohort found that the MHO group had the lowest risk of AD (HR, 0.87; 95% CI, 0.86–0.88) compared to the MHNO group [66]. Similarly, in a longitudinal study of 1,199 Europeans (drawn from the Alzheimer's Disease Neuroimaging Initiative database) who were initially free of AD, the risk of AD among elderly obese individuals was significantly reduced after adjusting for metabolic status (HR, 0.70; 95% CI, 0.56–0.89) [65]. Our findings, which were obtained from a Korean nationwide health examination cohort, are consistent with those of prior research, which found that MHO individuals had a much lower risk of AD (HR, 0.73; 95% CI, 0.65–0.81). Furthermore, we discovered that AD risk was significantly dependent on changes in BMI and metabolic health phenotypes, as well as baseline status. Maintaining the MHO phenotype, in particular, was associated with a much lower chance of developing AD even compared to the MHNO phenotype (HR, 0.62; 95% CI, 0.50–0.77). Among MUO participants at baseline, those who converted to the MUNO phenotype had a higher risk of AD, but those who transitioned to the MHO phenotype were protected from AD development (HR, 0.62; 95% CI, 0.50–0.78). In contrast, our additional analyses revealed that the MHO phenotype had no protective impact against vascular dementia. The pathophysiology of vascular dementia is most likely linked to stroke, as vascular insufficiency is the predominant pathophysiologic mechanism underlying both stroke and vascular dementia [67]. Previous research has found that MHO subjects have a similar or slightly higher risk of stroke than MHNO patients [19,28,68–71]. Because the pathophysiology of vascular dementia differs from that of AD, the effects of fat on vascular dementia may differ from those of obesity on AD.
- In summary, the MHO phenotype has distinct clinical consequences for a variety of outcomes, which are largely different from those of MUO. Furthermore, the clinical implications of MHO should also be considered in a context in which metabolic health is a transitory, not a permanent, state, as this aspect of MHO phenotype significantly impacts the clinical outcomes (Table 1) [19,43,51,59,72]. In general, recovery or maintenance of metabolic health could lead to a more favorable prognosis; therefore, clinicians should counsel obese patients about metabolic fitness to help prevent the development of obesity-related comorbidities.
PERSPECTIVES ON THE MUNO PHENOTYPE
- For a long time, the critical finding of very high CV risk and mortality in subjects with MUNO was underappreciated in research on the cardiometabolic risk of individuals according to the obese metabolic health phenotype [73–77]. MUNO patients had a considerably higher risk of all-cause mortality, CKD, and colorectal cancer in our studies [19,51,59]. Moreover, MHO individuals who changed to the MUNO status had substantially higher all-cause mortality than the stable MHO group, indicating the deleterious nature of this phenotype. Stefan et al. [78] recently summarized the features of the MUNO phenotype; these lean subjects with metabolic risk factors have an unfavorable body fat distribution, such as a low leg fat mass, visceral obesity, or fatty liver. This phenotype is also characterized by decreased insulin secretion capacity and increased insulin resistance, as well as poor cardiorespiratory fitness and carotid atherosclerosis [78]. These findings urge clinicians to develop clinical interventions to improve metabolic health in these individuals, despite not being classed as traditional obesity. Indeed, well-defined phenotyping strategies will help to precisely understand the pathophysiology of cardiometabolic disease, allowing for targeted lifestyle and pharmacological interventions to prevent adverse outcomes, including the ultimate goal of reducing mortality.
CONCLUSIONS
- In the modern era of precision medicine, the heterogeneity of clinical outcomes in obese people has significant implications. As the likelihood of developing cardiometabolic diseases is reliant on the presence of metabolic abnormalities, a definition of obesity based purely on BMI status does not provide sufficient insight into current and future health outcomes. Previous research has demonstrated that those with MHO had a lower risk of future CVD, CKD, cancer, and mortality than people with MUO; nevertheless, an elevated risk for the majority of those outcomes was observed in MHO people compared to those with MHNO. Obesity appears to be protective against AD, particularly in the absence of metabolic abnormalities. Currently, there are no randomized, controlled trials on the effectiveness of obesity treatment between individuals with MHO and MUO; however, a substantial amount of evidence suggests that maintenance or recovery of metabolic fitness in obese individuals protects them from obesity-related adverse outcomes. Further epidemiological research may discover modifiable risk factors and therapeutic interventions to prevent conversions from MHO to MUO, thereby affecting the future cardiometabolic fate of obese patients.
ARTICLE INFORMATION
-
Ethical statements
Not applicable.
-
Conflicts of interest
The authors have no conflicts of interest to declare.
-
Funding
None.
-
Author contributions
Conceptualization: CHJ; Investigation: all authors; Writing–original draft: YKC; Writing–review & editing: CHJ.
All authors read and approved the final manuscript.
Fig. 1.Risk factors for transition from metabolically healthy obesity to metabolically unhealthy obesity.
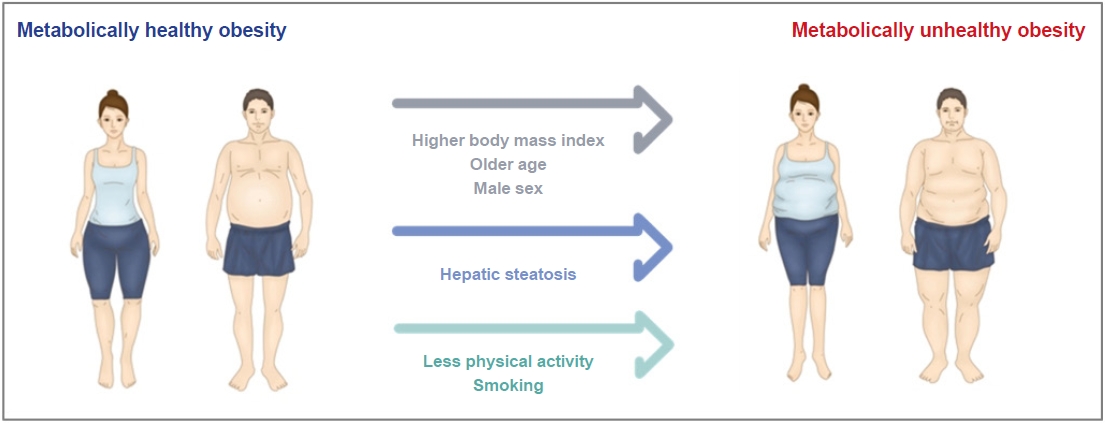
Table 1.Heterogeneous outcomes of the MHO phenotypea) according to the phenotypic transitions over time
|
Variable |
Mortalityb)
|
CV eventsb)
|
T2Dc)
|
CKDd)
|
CRCe)
|
ADf)
|
|
Study |
Cho et al. [19] |
Cho et al. [19] |
Wang et al. [43] |
Cho et al. [51] |
Cho et al. [59] |
Cho et al. [72] |
|
Baseline |
|
|
|
|
|
|
|
MHNO |
1 (Reference) |
1 (Reference) |
1 (Reference) |
1 (Reference) |
1 (Reference) |
1 (Reference) |
|
MHO |
0.86 (0.79–0.93) |
1.14 (1.05–1.24) |
1.94 (1.33–2.81) |
1.23 (1.12–1.36) |
1.14 (1.04–1.26) |
0.73 (0.65–0.81) |
|
Transition |
|
|
|
|
|
|
|
Stable MHNO |
NA |
NA |
1 (Reference) |
1 (Reference) |
1 (Reference) |
NA |
|
MHO to MHNO |
1.18 (0.87–1.61) |
1.02 (0.74–1.40) |
NA |
0.98 (0.72–1.32) |
NA |
0.98 (0.71–1.34) |
|
Stable MHO |
1 (Reference) |
1 (Reference) |
0.31 (0.10–0.97) |
1.23 (1.04–1.44) |
0.97 (0.83–1.14) |
0.62 (0.50–0.77) |
|
MHO to MUNO |
1.96 (1.45–2.65) |
1.23 (0.86–1.78) |
4.52 (1.28–16.04) |
1.60 (1.16–2.20) |
NA |
1.23 (0.86–1.76) |
|
MHO to MUO |
1.19 (0.96–1.48) |
1.24 (1.00–1.54) |
3.54 (1.80–6.96) |
1.68 (1.45–1.96) |
1.34 (1.15–1.57) |
0.97 (0.81–1.17) |
REFERENCES
- 1. Abdelaal M, le Roux CW, Docherty NG. Morbidity and mortality associated with obesity. Ann Transl Med 2017;5:161. ArticlePubMedPMC
- 2. Arroyo-Johnson C, Mincey KD. Obesity epidemiology worldwide. Gastroenterol Clin North Am 2016;45:571–9.ArticlePubMedPMC
- 3. Yang YS, Han BD, Han K, Jung JH, Son JW; Taskforce Team of the Obesity Fact Sheet of the Korean Society for the Study of Obesity. Obesity Fact Sheet in Korea, 2021: trends in obesity prevalence and obesity-related comorbidity incidence stratified by age from 2009 to 2019. J Obes Metab Syndr 2022;31:169–77.ArticlePubMedPMC
- 4. WHO Expert Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet 2004;363:157–63.ArticlePubMed
- 5. Nam GE, Kim YH, Han K, Jung JH, Rhee EJ, Lee WY, et al. Obesity Fact Sheet in Korea, 2020: prevalence of obesity by obesity class from 2009 to 2018. J Obes Metab Syndr 2021;30:141–8.ArticlePubMedPMC
- 6. Jung CH, Lee WJ, Song KH. Metabolically healthy obesity: a friend or foe? Korean J Intern Med 2017;32:611–21.ArticlePubMedPMCPDF
- 7. Phillips CM. Metabolically healthy obesity: definitions, determinants and clinical implications. Rev Endocr Metab Disord 2013;14:219–27.ArticlePubMedPDF
- 8. Stefan N, Haring HU, Hu FB, Schulze MB. Metabolically healthy obesity: epidemiology, mechanisms, and clinical implications. Lancet Diabetes Endocrinol 2013;1:152–62.ArticlePubMed
- 9. Samocha-Bonet D, Dixit VD, Kahn CR, Leibel RL, Lin X, Nieuwdorp M, et al. Metabolically healthy and unhealthy obese: the 2013 Stock Conference report. Obes Rev 2014;15:697–708.ArticlePubMedPMC
- 10. Bluher M. Are metabolically healthy obese individuals really healthy? Eur J Endocrinol 2014;171:R209–19.ArticlePubMed
- 11. Hinnouho GM, Czernichow S, Dugravot A, Batty GD, Kivimaki M, Singh-Manoux A. Metabolically healthy obesity and risk of mortality: does the definition of metabolic health matter? Diabetes Care 2013;36:2294–300.ArticlePubMedPMC
- 12. Hinnouho GM, Czernichow S, Dugravot A, Nabi H, Brunner EJ, Kivimaki M, et al. Metabolically healthy obesity and the risk of cardiovascular disease and type 2 diabetes: the Whitehall II cohort study. Eur Heart J 2015;36:551–9.ArticlePubMedPMC
- 13. Bluher M. Metabolically healthy obesity. Endocr Rev 2020;41:bnaa004. ArticlePubMedPMC
- 14. Bray GA, Kim KK, Wilding JH; World Obesity Federation. Obesity: a chronic relapsing progressive disease process. A position statement of the World Obesity Federation. Obes Rev 2017;18:715–23.ArticlePubMedPDF
- 15. Bray GA, Heisel WE, Afshin A, Jensen MD, Dietz WH, Long M, et al. The science of obesity management: an Endocrine Society scientific statement. Endocr Rev 2018;39:79–132.ArticlePubMedPMC
- 16. Mongraw-Chaffin M, Foster MC, Anderson CA, Burke GL, Haq N, Kalyani RR, et al. Metabolically healthy obesity, transition to metabolic syndrome, and cardiovascular risk. J Am Coll Cardiol 2018;71:1857–65.ArticlePubMedPMC
- 17. Lin H, Zhang L, Zheng R, Zheng Y. The prevalence, metabolic risk and effects of lifestyle intervention for metabolically healthy obesity: a systematic review and meta-analysis: a PRISMA-compliant article. Medicine (Baltimore) 2017;96:e8838.ArticlePubMedPMC
- 18. Soriguer F, Gutierrez-Repiso C, Rubio-Martin E, Garcia-Fuentes E, Almaraz MC, Colomo N, et al. Metabolically healthy but obese, a matter of time? Findings from the prospective Pizarra study. J Clin Endocrinol Metab 2013;98:2318–25.ArticlePubMed
- 19. Cho YK, Kang YM, Yoo JH, Lee J, Park JY, Lee WJ, et al. Implications of the dynamic nature of metabolic health status and obesity on risk of incident cardiovascular events and mortality: a nationwide population-based cohort study. Metabolism 2019;97:50–6.ArticlePubMed
- 20. Guo F, Garvey WT. Cardiometabolic disease risk in metabolically healthy and unhealthy obesity: stability of metabolic health status in adults. Obesity (Silver Spring) 2016;24:516–25.ArticlePubMedPMCPDF
- 21. Hashimoto Y, Hamaguchi M, Fukuda T, Ohbora A, Kojima T, Fukui M. Fatty liver as a risk factor for progression from metabolically healthy to metabolically abnormal in non-overweight individuals. Endocrine 2017;57:89–97.ArticlePubMedPDF
- 22. Moussa O, Arhi C, Ziprin P, Darzi A, Khan O, Purkayastha S. Fate of the metabolically healthy obese-is this term a misnomer? A study from the Clinical Practice Research Datalink. Int J Obes (Lond) 2019;43:1093–101.ArticlePubMedPDF
- 23. Cui Z, Truesdale KP, Bradshaw PT, Cai J, Stevens J. Three-year weight change and cardiometabolic risk factors in obese and normal weight adults who are metabolically healthy: the atherosclerosis risk in communities study. Int J Obes (Lond) 2015;39:1203–8.ArticlePubMedPDF
- 24. Espinosa De Ycaza AE, Donegan D, Jensen MD. Long-term metabolic risk for the metabolically healthy overweight/obese phenotype. Int J Obes (Lond) 2018;42:302–9.ArticlePubMedPMCPDF
- 25. Appleton SL, Seaborn CJ, Visvanathan R, Hill CL, Gill TK, Taylor AW, et al. Diabetes and cardiovascular disease outcomes in the metabolically healthy obese phenotype: a cohort study. Diabetes Care 2013;36:2388–94.ArticlePubMedPMC
- 26. Lavie CJ, De Schutter A, Milani RV. Healthy obese versus unhealthy lean: the obesity paradox. Nat Rev Endocrinol 2015;11:55–62.ArticlePubMedPDF
- 27. Mørkedal B, Vatten LJ, Romundstad PR, Laugsand LE, Janszky I. Risk of myocardial infarction and heart failure among metabolically healthy but obese individuals: HUNT (Nord-Trøndelag Health Study), Norway. J Am Coll Cardiol 2014;63:1071–8.ArticlePubMed
- 28. Caleyachetty R, Thomas GN, Toulis KA, Mohammed N, Gokhale KM, Balachandran K, et al. Metabolically healthy obese and incident cardiovascular disease events among 3.5 million men and women. J Am Coll Cardiol 2017;70:1429–37.ArticlePubMed
- 29. Bell JA, Hamer M, Batty GD, Singh-Manoux A, Sabia S, Kivimaki M. Incidence of metabolic risk factors among healthy obese adults: 20-year follow-up. J Am Coll Cardiol 2015;66:871–3.ArticlePubMedPMC
- 30. Eckel N, Li Y, Kuxhaus O, Stefan N, Hu FB, Schulze MB. Transition from metabolic healthy to unhealthy phenotypes and association with cardiovascular disease risk across BMI categories in 90 257 women (the Nurses' Health Study): 30 year follow-up from a prospective cohort study. Lancet Diabetes Endocrinol 2018;6:714–24.ArticlePubMed
- 31. Kouvari M, Panagiotakos DB, Yannakoulia M, Georgousopoulou E, Critselis E, Chrysohoou C, et al. Transition from metabolically benign to metabolically unhealthy obesity and 10-year cardiovascular disease incidence: the ATTICA cohort study. Metabolism 2019;93:18–24.ArticlePubMed
- 32. Goyal A, Nimmakayala KR, Zonszein J. Is there a paradox in obesity? Cardiol Rev 2014;22:163–70.ArticlePubMedPMC
- 33. Teunkens A, Van de Velde M, Vermeulen K, Van Loon P, Bogaert G, Fieuws S, et al. Dorsal penile nerve block for circumcision in pediatric patients: a prospective, observer-blinded, randomized controlled clinical trial for the comparison of ultrasound-guided vs landmark technique. Paediatr Anaesth 2018;28:703–9.ArticlePubMedPDF
- 34. Elagizi A, Kachur S, Lavie CJ, Carbone S, Pandey A, Ortega FB, et al. An overview and update on obesity and the obesity paradox in cardiovascular diseases. Prog Cardiovasc Dis 2018;61:142–50.ArticlePubMed
- 35. GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020;396:1204–22.ArticlePubMedPMC
- 36. International Diabetes Federation (IDF). IDF diabetes atlas. 10th ed. Brussels, IDF; 2021.
- 37. Zheng Y, Ley SH, Hu FB. Global aetiology and epidemiology of type 2 diabetes mellitus and its complications. Nat Rev Endocrinol 2018;14:88–98.ArticlePubMedPDF
- 38. Bell JA, Kivimaki M, Hamer M. Metabolically healthy obesity and risk of incident type 2 diabetes: a meta-analysis of prospective cohort studies. Obes Rev 2014;15:504–15.ArticlePubMedPMCPDF
- 39. Hashimoto Y, Hamaguchi M, Tanaka M, Obora A, Kojima T, Fukui M. Metabolically healthy obesity without fatty liver and risk of incident type 2 diabetes: a meta-analysis of prospective cohort studies. Obes Res Clin Pract 2018;12:4–15.ArticlePubMed
- 40. Twig G, Afek A, Derazne E, Tzur D, Cukierman-Yaffe T, Gerstein HC, et al. Diabetes risk among overweight and obese metabolically healthy young adults. Diabetes Care 2014;37:2989–95.ArticlePubMedPDF
- 41. Guo F, Garvey WT. Development of a weighted cardiometabolic disease staging (CMDS) system for the prediction of future diabetes. J Clin Endocrinol Metab 2015;100:3871–7.ArticlePubMedPMC
- 42. Guo F, Moellering DR, Garvey WT. The progression of cardiometabolic disease: validation of a new cardiometabolic disease staging system applicable to obesity. Obesity (Silver Spring) 2014;22:110–8.ArticlePubMedPMCPDF
- 43. Wang B, Zhang M, Wang S, Wang C, Wang J, Li L, et al. Dynamic status of metabolically healthy overweight/obesity and metabolically unhealthy and normal weight and the risk of type 2 diabetes mellitus: a cohort study of a rural adult Chinese population. Obes Res Clin Pract 2018;12:61–71.ArticlePubMed
- 44. Wahba IM, Mak RH. Obesity and obesity-initiated metabolic syndrome: mechanistic links to chronic kidney disease. Clin J Am Soc Nephrol 2007;2:550–62.ArticlePubMed
- 45. Jung CH, Lee MJ, Kang YM, Hwang JY, Kim EH, Park JY, et al. The risk of chronic kidney disease in a metabolically healthy obese population. Kidney Int 2015;88:843–50.ArticlePubMed
- 46. Ruster C, Wolf G. Adipokines promote chronic kidney disease. Nephrol Dial Transplant 2013;28 Suppl 4:iv8–14.ArticlePubMed
- 47. Chang Y, Ryu S, Choi Y, Zhang Y, Cho J, Kwon MJ, et al. Metabolically healthy obesity and development of chronic kidney disease: a cohort study. Ann Intern Med 2016;164:305–12.ArticlePubMed
- 48. Nam KH, Yun HR, Joo YS, Kim J, Lee S, Lee C, et al. Changes in obese metabolic phenotypes over time and risk of incident chronic kidney disease. Diabetes Obes Metab 2018;20:2778–91.ArticlePubMedPDF
- 49. Hashimoto Y, Tanaka M, Okada H, Senmaru T, Hamaguchi M, Asano M, et al. Metabolically healthy obesity and risk of incident CKD. Clin J Am Soc Nephrol 2015;10:578–83.ArticlePubMedPMC
- 50. Nashar K, Egan BM. Relationship between chronic kidney disease and metabolic syndrome: current perspectives. Diabetes Metab Syndr Obes 2014;7:421–35.ArticlePubMedPMC
- 51. Cho YK, Lee J, Kim HS, Park JY, Lee WJ, Kim YJ, et al. Impact of transition in metabolic health and obesity on the incident chronic kidney disease: a nationwide cohort study. J Clin Endocrinol Metab 2020;105:dgaa033. ArticlePubMedPDF
- 52. Calle EE, Kaaks R. Overweight, obesity and cancer: epidemiological evidence and proposed mechanisms. Nat Rev Cancer 2004;4:579–91.ArticlePubMedPDF
- 53. Ma Y, Yang Y, Wang F, Zhang P, Shi C, Zou Y, et al. Obesity and risk of colorectal cancer: a systematic review of prospective studies. PLoS One 2013;8:e53916.ArticlePubMedPMC
- 54. Murphy N, Cross AJ, Abubakar M, Jenab M, Aleksandrova K, Boutron-Ruault MC, et al. A nested case-control study of metabolically defined body size phenotypes and risk of colorectal cancer in the European Prospective Investigation into Cancer and Nutrition (EPIC). PLoS Med 2016;13:e1001988.ArticlePubMedPMC
- 55. Yun KE, Chang Y, Jung HS, Kim CW, Kwon MJ, Park SK, et al. Impact of body mass index on the risk of colorectal adenoma in a metabolically healthy population. Cancer Res 2013;73:4020–7.ArticlePubMedPDF
- 56. Kim JY, Park DI, Yu J, Jung YS, Park JH, Kim HJ, et al. Increased risk of advanced colorectal neoplasia among Korean men with metabolic abnormality and obesity. Clin Gastroenterol Hepatol 2016;14:1310–6.ArticlePubMed
- 57. Ko SH, Baeg MK, Ko SY, Jung HS, Kim P, Choi MG. Obesity and metabolic unhealthiness have different effects on colorectal neoplasms. J Clin Endocrinol Metab 2017;102:2762–9.ArticlePubMed
- 58. Shin CM, Han K, Lee DH, Choi YJ, Kim N, Park YS, et al. Association among obesity, metabolic health, and the risk for colorectal cancer in the general population in Korea using the National Health Insurance Service-National Sample Cohort. Dis Colon Rectum 2017;60:1192–200.ArticlePubMed
- 59. Cho YK, Lee J, Kim HS, Park JY, Lee WJ, Kim YJ, et al. Metabolic health is a determining factor for incident colorectal cancer in the obese population: a nationwide population-based cohort study. Cancer Med 2021;10:220–9.ArticlePubMedPDF
- 60. Yu JH, Han K, Park S, Cho H, Lee DY, Kim JW, et al. Incidence and risk factors for dementia in type 2 diabetes mellitus: a nationwide population-based study in Korea. Diabetes Metab J 2020;44:113–24.ArticlePubMedPMCPDF
- 61. Dahl AK, Lopponen M, Isoaho R, Berg S, Kivela SL. Overweight and obesity in old age are not associated with greater dementia risk. J Am Geriatr Soc 2008;56:2261–6.ArticlePubMed
- 62. Emmerzaal TL, Kiliaan AJ, Gustafson DR. 2003-2013: a decade of body mass index, Alzheimer's disease, and dementia. J Alzheimers Dis 2015;43:739–55.ArticlePubMed
- 63. Fitzpatrick AL, Kuller LH, Lopez OL, Diehr P, O'Meara ES, Longstreth WT Jr, et al. Midlife and late-life obesity and the risk of dementia: cardiovascular health study. Arch Neurol 2009;66:336–42.ArticlePubMedPMC
- 64. Hughes TF, Borenstein AR, Schofield E, Wu Y, Larson EB. Association between late-life body mass index and dementia: the Kame Project. Neurology 2009;72:1741–6.ArticlePubMedPMC
- 65. Ma LZ, Huang YY, Wang ZT, Li JQ, Hou XH, Shen XN, et al. Metabolically healthy obesity reduces the risk of Alzheimer's disease in elders: a longitudinal study. Aging (Albany NY) 2019;11:10939–51.ArticlePubMedPMC
- 66. Lee JY, Han K, Han E, Kim G, Cho H, Kim KJ, et al. Risk of incident dementia according to metabolic health and obesity status in late life: a population-based cohort study. J Clin Endocrinol Metab 2019;104:2942–52.ArticlePubMed
- 67. Kalaria RN. The pathology and pathophysiology of vascular dementia. Neuropharmacology 2018;134(Pt B):226–39.Article
- 68. Sanchez-Inigo L, Navarro-Gonzalez D, Fernandez-Montero A, Pastrana-Delgado J, Martinez JA. Risk of incident ischemic stroke according to the metabolic health and obesity states in the Vascular-Metabolic CUN cohort. Int J Stroke 2017;12:187–91.ArticlePubMedPDF
- 69. Byun AR, Kwon S, Lee SW, Shim KW, Lee HS. Metabolic health is more closely associated with prevalence of cardiovascular diseases or stroke than obesity: a cross-sectional study in Korean populations. Medicine (Baltimore) 2016;95:e3902.ArticlePubMedPMC
- 70. Li Z, Guo X, Liu Y, Zhang N, Chang Y, Chen Y, et al. Metabolism rather than obesity is associated with ischemic stroke: a cross-sectional study in rural Northeastern China. Springerplus 2016;5:1419. ArticlePubMedPMCPDF
- 71. Lee HJ, Choi EK, Lee SH, Kim YJ, Han KD, Oh S. Risk of ischemic stroke in metabolically healthy obesity: a nationwide population-based study. PLoS One 2018;13:e0195210.ArticlePubMedPMC
- 72. Cho YK, Lee J, Kim HS, Park JY, Lee WJ, Kim YJ, et al. The risk of Alzheimer's disease according to dynamic changes in metabolic health and obesity: a nationwide population-based cohort study. Aging (Albany NY) 2021;13:16974–89.ArticlePubMedPMC
- 73. Stefan N. Metabolically healthy and unhealthy normal weight and obesity. Endocrinol Metab (Seoul) 2020;35:487–93.ArticlePubMedPMCPDF
- 74. Kramer CK, Zinman B, Retnakaran R. Are metabolically healthy overweight and obesity benign conditions? A systematic review and meta-analysis. Ann Intern Med 2013;159:758–69.ArticlePubMed
- 75. Hamer M, Stamatakis E. Metabolically healthy obesity and risk of all-cause and cardiovascular disease mortality. J Clin Endocrinol Metab 2012;97:2482–8.ArticlePubMedPMC
- 76. Eckel N, Meidtner K, Kalle-Uhlmann T, Stefan N, Schulze MB. Metabolically healthy obesity and cardiovascular events: a systematic review and meta-analysis. Eur J Prev Cardiol 2016;23:956–66.ArticlePubMedPDF
- 77. Lassale C, Tzoulaki I, Moons KG, Sweeting M, Boer J, Johnson L, et al. Separate and combined associations of obesity and metabolic health with coronary heart disease: a pan-European case-cohort analysis. Eur Heart J 2018;39:397–406.ArticlePubMedPMC
- 78. Stefan N, Schick F, Haring HU. Causes, characteristics, and consequences of metabolically unhealthy normal weight in humans. Cell Metab 2017;26:292–300.ArticlePubMed
Citations
Citations to this article as recorded by

 , Chang Hee Jung1,2
, Chang Hee Jung1,2

 PubReader
PubReader ePub Link
ePub Link Cite
Cite