ABSTRACT
-
Background
- Although postmenopausal women are well known to have a high prevalence of hypertension, it is unclear whether menopause itself increases blood pressure independently from the known risk factors of hypertension. This study sought to determine whether an association exists between reproductive aging and an increased risk of hypertension among Korean women.
-
Methods
- This cross-sectional study used baseline data from 5,456 women aged 30 to 64 years who participated in the Cardiovascular and Metabolic Diseases Etiology Research Center study in Korea from 2013 to 2018. The participants’ stage of reproductive aging was assessed by a questionnaire and categorized as premenopause, perimenopause, and postmenopause. Multiple logistic regression models were used to analyze the association between menopausal status and hypertension after adjusting for age, education level, marital status, employment, household income, smoking, drinking, physical activity, body mass index, and hormone replacement therapy use.
-
Results
- The prevalence of hypertension increased with reproductive aging: 9.8% in premenopause, 25.2% in perimenopause, and 27.7% in postmenopause. The adjusted odds ratio (95% confidence interval) for having hypertension was 1.70 (1.07–2.72) for perimenopausal women and 1.14 (0.88–1.48) for postmenopausal women, compared to premenopausal women.
-
Conclusions
- Our study shows that perimenopausal women are at high risk of developing hypertension. Since the menopausal transition may last months or years, blood pressure monitoring and early interventions are crucial for not only postmenopausal women, but also those in the transition.
-
Keywords: Menopause; Perimenopause; Aging; Hypertension
INTRODUCTION
- Elevated blood pressure (BP) is the most prevalent risk factor for cardiovascular morbidity and mortality worldwide, although it is modifiable [1,2]. The widespread use of antihypertensive medication and global efforts to alleviate the impact of hypertension have resulted in either a stabilization or a slight decrease in mean BP globally [3,4]. The prevalence of hypertension, however, has increased worldwide [1]. In Korea, 28% of adults were estimated to have hypertension in 2019, and the increase in the prevalence was more prominent in the elderly, particularly in women [5].
- Although BP is likely to increase with aging in both men and women, the sex difference is reversed when women go through menopause [6]. Premenopausal women have a lower prevalence of hypertension than men of the same age, but hypertension increases rapidly after menopause, and women have a higher prevalence of hypertension than men among the elderly [7–9]. These findings suggest that menopause plays a notable role in hypertension.
- However, there have been inconsistent findings on whether menopause itself affects hypertension. Some studies have demonstrated a significant relationship between menopause and hypertension [10]. In these studies, both systolic and diastolic BP were associated with menopause after adjusting for age and body mass index (BMI) [11–13]. Postmenopausal women taking hormone replacement therapy had a lower increase in BP than nonusers [14], implying that changes and deficits in sex hormones during menopause play a significant role in hypertension. Other studies, by contrast, suggested that the association is mainly explained by postmenopausal changes in established risk factors [10,15,16]. For instance, the higher risk of hypertension in the postmenopausal group lost its significance after controlling for age, smoking, BMI, and the presence of metabolic syndrome [10,15,16]. A longitudinal study reported that menopause appeared to have a protective effect on BP elevation due to aging [17]. In this context, this study aimed to determine whether an association exists between reproductive aging and hypertension among Korean women.
METHODS
- Ethical statement
- This study used the baseline data of the Cardiovascular and Metabolic Diseases Etiology Research Center (CMERC) cohort study, that was approved by the Institutional Review Boards of Severance Hospital, Yonsei University Health System, Seoul, Korea (No. 4-2013-0661) and Ajou University Hospital, Suwon, Korea (No. AJIRB-BMR-SUR-13-272). Written informed consent was obtained from all participants prior to the baseline survey.
- Study participants
- This cross-sectional study used baseline data from the CMERC study. The CMERC study is a multicenter prospective study conducted to obtain valuable evidence for the prevention and management of cardiovascular disease. A total of 8,697 individuals free from myocardial infarction, heart failure, stroke, or recent cancer were recruited at baseline from 2013 to 2018. The detailed information on the study has been previously published in separate articles [18,19]. After exclusion of male participants (n=3,060) and those with missing data for related variables (n=181), 5,456 female participants aged 30 to 64 were included in our analyses.
- Measurements
- The stage of reproductive aging was assessed by a questionnaire. The definitions of menstruation adopted the 2001 Stages of Reproductive Aging Workshop criteria [20], which divide adult female life into three broad phases: premenopause (reproductive), perimenopause (menopausal transition), and postmenopause [2]. Those who had menstruated in the last 3 months were classified as premenopausal regardless of the regularity of menstruation. If participants had menstruated occasionally over the past 12 months but eventually stopped menstruating in the most recent 3 months, they were considered perimenopausal. Postmenopause was defined as the absence of menstruation in the past 12 months or more or a history of hysterectomy or oophorectomy. Age at menopause was also collected and used to calculate the period after menopause.
- BP was measured in the right arm except when doing so was not possible, such as in participants with a history of breast cancer surgery. Participants rested for at least 5 minutes in a seated position before the first measurement. Measurements were conducted three times at 2-minute intervals using an automated oscillometric device (HEM-7080; Omron Health, Matsusaka, Japan) under a standardized protocol. This study used the average of the second and third values. We defined hypertension (also referred to herein as total hypertension) when the definition of systolic hypertension, diastolic hypertension, or treated hypertension was satisfied. Systolic hypertension was defined as a mean systolic BP ≥140 mmHg; diastolic hypertension as a mean diastolic BP ≥90 mmHg; and treated hypertension as being on antihypertensive medication. The subtypes of hypertension were not mutually exclusive. Based on the literature, we selected potential confounders that included age, socioeconomic status (e.g., education level and annual household income), health-related behaviors (smoking, drinking, and physical activity), BMI, and hormone replacement therapy.
- Statistical analysis
- The general characteristics of the three groups (premenopause, perimenopause, and postmenopause) were presented as mean values with the standard deviation for continuous variables, and as the number of cases with percentage for categorical variables. Comparisons were conducted using analysis of variance or the chi-square test, correspondingly. Simple and multiple logistic regression models were used to estimate the association between the stage of reproductive aging and hypertension before and after controlling for potential confounders. Model 1 controlled for education level, marital status, employment, household income, smoking, drinking, physical activity, BMI, and hormone replacement therapy use, and model 2 was adjusted for age in addition to all covariates used in model 1. In a sub-analysis, postmenopausal women were divided into six groups by units of 3 years from menopause. By doing so, their risk of raised BP was estimated according to the time elapsed since menopause. A two-sided P-value lower than 0.05 was considered to indicate statistical significance. All analyses were performed using SAS ver. 9.4 (SAS Institute Inc., Cary, NC, USA).
RESULTS
- Participants’ characteristics
- Among 5,456 participants, 1,894 were premenopausal, 3,443 were postmenopausal, and 119 were in the menopausal transition. The menopausal participants were older (mean±standard deviation; 42.81±6.37 years in the premenopausal group; 50.80±4.03 years in the perimenopausal group; 56.88±4.21 years in the postmenopausal group), more likely to have an educational level of middle school or lower (3.5% in the premenopausal group; 11.8% in the perimenopausal group; 27.1% in the postmenopausal group), and more likely to be obese (23.2% in the premenopausal group; 29.4% in the perimenopausal group; 31.2% in the postmenopausal group) than the premenopausal and perimenopausal groups (Table 1).
- Association between hypertension and the stage of reproductive aging
- The prevalence of total hypertension was higher in postmenopause (27.7%), than in premenopause (9.8%) or perimenopause (25.2%). The prevalence of treated hypertension increased with the stage of reproductive aging. Systolic and diastolic hypertension, however, were highest among women in the menopausal transition (10.9% and 9.2%, respectively) (Table 2).
-
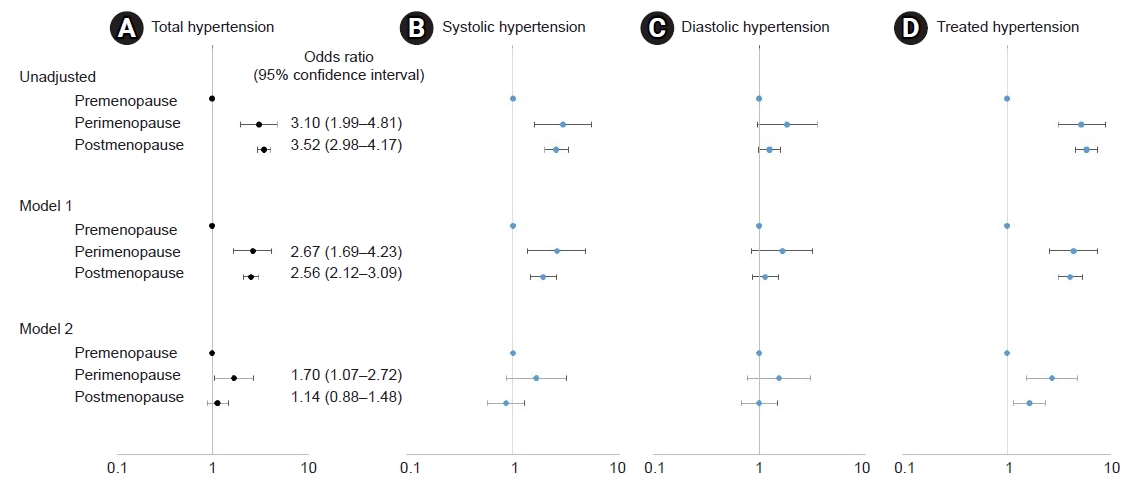
Fig. 1 shows the unadjusted and adjusted odds ratios of hypertension and its subtypes compared to the premenopausal group. The unadjusted odds ratio (95% confidence interval) for total hypertension was 3.10 (1.99–4.81) in perimenopausal women and 3.52 (2.98–4.17) in postmenopausal women. Treated hypertension showed an increasing unadjusted risk with reproductive aging, but those in the menopausal transition seemed to have the highest risk for systolic and diastolic hypertension. Two models were used to examine the adjusted odds ratios. Model 1 controlled for all related variables except age. The risks of systolic and diastolic hypertension were consistently higher in perimenopause. The odds ratio of being on antihypertensive medication became the greatest in perimenopause after adjustment. Model 2 was fully adjusted, including age. The finding that perimenopausal women had the highest odds ratio was persistent in this model (Table S1).
- To determine how the increased risk of hypertension in perimenopause changed with time after menopause, the postmenopausal period was calculated, and postmenopausal participants were divided into six groups. As shown in Fig. 2, the risk of systolic hypertension was highest during menopause and decreased immediately after menopause, but gradually increased again over time. The risk of diastolic hypertension was highest during menopause and continued to decrease over time. However, we could not fully assess the age-independent effects of postmenopausal duration on hypertension, because the sample size of this study was not large enough and the duration of the postmenopausal period was closely correlated with age.
DISCUSSION
- In this study, we observed that women going through the menopausal transition had a higher prevalence of hypertension than premenopausal and postmenopausal women. Menopause typically occurs between the ages of 49 and 52 years [21]. The prevalence of hypertension also increases with age [22]. Therefore, age may affect both menopause and the development of hypertension. It is noteworthy that perimenopausal women had a higher risk of hypertension than postmenopausal women, even after adjustment for age.
- Although there is little research directly investigating the mechanism linking perimenopause and elevated BP in humans, a mechanism can be inferred from studies on postmenopausal hypertension and on animal models comparable to human perimenopause. The mechanism of postmenopausal hypertension was explained by changes in the estrogen/androgen ratio, along with changes in other established risk factors of hypertension [10]. Menopause is accompanied by a deficit of estradiol and a decrease in the estrogen-to-testosterone ratio, resulting in a disturbance of the renin-angiotensin system, endothelial dysfunction, and increased BMI. These lead to increased levels of angiotensin Ⅱ, oxidative stress, and endothelin, but decreased levels of endogenous nitric oxide, and all of these changes contribute to increases in renal vasoconstriction, causing hypertension [8,10,23,24]. Furthermore, mouse models mimicking the characteristics of human perimenopause (accelerated ovarian failure in estrogen receptor β reporter mice) suggested that estrogen receptor β signaling plays a significant role in BP regulation. An estrogen receptor β agonist suppressed the increase in BP in mice with neurogenic hypertension induced by angiotensin Ⅱ, and deletion of estrogen receptor β produced a phenotype with sensitivity to hypertension [25,26]. In this context, fluctuations of sex hormones and their impact on angiotensin Ⅱ among perimenopausal women may at least partially explain the increased risk of hypertension.
- This study has some strengths and limitations. Considering that most previous studies on the association between menopause and hypertension divided participants into only two groups (nonmenopausal and menopausal), a strength of our study is that it took perimenopausal women into account and highlighted that they showed the highest level of risk. We were able to adjust for most known risk factors including socioeconomic status, lifestyle factors, and hormone replacement therapy use, thereby minimizing confounding effects. Despite these advantages, some limitations should be acknowledged. First, we measured BP in the clinic with a single visit. The data used in this study did not permit us to distinguish “white coat” hypertension or “masked” hypertension, although the average of the second and third measurements was used, with at least a 5-minute rest preceding the measurements. Given that out-of-office BP is recommended to evaluate white coat or masked hypertension [27–29], the use of only in-office BP measurements may have affected our findings. Second, information on reproductive aging was obtained by self-report, so the possibility of misclassification cannot be excluded. Third, although we controlled for most of the major risk factors for hypertension, there remains the possibility of residual confounding due to measurement errors and/or unmeasured confounders.
- In conclusion, perimenopausal women were found to be at risk of developing transient or persistent hypertension. While recognizing that elevated BP among women in the menopausal transition might be transient or persist, we need to be cautious not to overlook the hypertension risk of perimenopausal women by focusing only on managing other menopausal symptoms and complications. Considering that the menopausal transition may last months or years, BP monitoring and early interventions are crucial for not only postmenopausal women, but also those in the menopausal transition.
Supplementary Material
ARTICLE INFORMATION
-
Ethical statement
This study used the baseline data of the Cardiovascular and Metabolic Diseases Etiology Research Center (CMERC) cohort study, that was approved by the Institutional Review Boards of Severance Hospital, Yonsei University Health System, Seoul, Korea (No. 4-2013-0661) and Ajou University Hospital, Suwon, Korea (No. AJIRB-BMR-SUR-13-272). Written informed consent was obtained from all participants prior to the baseline survey.
-
Conflicts of interest
The authors have no conflicts of interest to declare.
-
Funding
None.
-
Author contributions
Conceptualization: EK; Formal analysis: EK; Supervision: HCK; Visualization: EK, YL; Writing–original draft: EK; Writing–review&editing: HCK. All authors read and approved the final manuscript.
Fig. 1.Association between stage of reproductive aging and hypertension. Model 1, adjusted for education level, marital status, employment, household income, smoking, drinking, physical activity, body mass index, and hormone replacement therapy use. Model 2, adjusted for age in addition to all covariates used in model 1. (A) Total hypertension, (B) systolic hypertension, (C) diastolic hypertension, and (D) treated hypertension.

Fig. 2.Association between years after menopause and hypertension. The risk of hypertension was adjusted for education level, marital status, employment, household income, smoking, drinking, physical activity, body mass index, and hormone replacement therapy use, not age. (A) Total hypertension, (B) systolic hypertension, (C) diastolic hypertension, and (D) treated hypertension.

Table 1.Characteristics of participants by the stage of reproductive aging
|
Variable |
Premenopause (n=1,894) |
Perimenopause (n=119) |
Postmenopause (n=3,443) |
P-valuea)
|
|
Age (yr) |
42.81±6.37 |
50.80±4.03 |
56.88±4.21 |
<0.001 |
|
Education level |
|
|
|
<0.001 |
|
Middle school or less |
67 (3.5) |
14 (11.8) |
934 (27.1) |
|
|
High school |
797 (42.1) |
61 (51.3) |
1,718 (49.9) |
|
|
University or beyond |
1,030 (54.4) |
44 (37.0) |
791 (23.0) |
|
|
Marital status |
|
|
|
0.051 |
|
Married |
1,613 (85.2) |
103 (86.5) |
2,849 (82.8) |
|
|
Divorced, widowed, or single |
281 (14.8) |
16 (13.5) |
594 (17.2) |
|
|
Working status |
|
|
|
<0.001 |
|
Working |
1,208 (63.8) |
85 (71.4) |
1,706 (49.5) |
|
|
Nonworking |
686 (36.2) |
34 (28.6) |
1,737 (50.5) |
|
|
Household annual income |
|
|
|
<0.001 |
|
Q1 |
199 (10.5) |
15 (12.6) |
782 (22.7) |
|
|
Q2 |
579 (30.6) |
31 (26.1) |
959 (27.9) |
|
|
Q3 |
581 (30.7) |
34 (28.6) |
781 (22.7) |
|
|
Q4 |
535 (28.3) |
39 (32.8) |
921 (26.7) |
|
|
Smoking |
|
|
|
<0.001 |
|
No |
1,709 (90.2) |
110 (92.4) |
3,315 (96.3) |
|
|
Ever |
185 (9.8) |
9 (7.6) |
128 (3.7) |
|
|
Current drinking |
|
|
|
<0.001 |
|
No |
524 (27.7) |
40 (33.6) |
1,464 (42.5) |
|
|
Yes |
1,370 (72.3) |
79 (66.4) |
1,979 (57.5) |
|
|
Body mass index |
|
|
|
<0.001 |
|
Normal or low body weight |
1,038 (54.8) |
49 (41.2) |
1,420 (41.2) |
|
|
Overweight |
416 (22.0) |
35 (29.4) |
950 (27.6) |
|
|
Obesity |
440 (23.2) |
35 (29.4) |
1,073 (31.2) |
|
|
Physical activity (MET score) |
|
|
|
<0.001 |
|
Inactive |
852 (45.0) |
56 (47.1) |
1,280 (37.2) |
|
|
Minimally active |
772 (40.7) |
44 (37.0) |
1,532 (44.5) |
|
|
Health-enhancing physical activity |
270 (14.3) |
19 (15.9) |
631 (18.3) |
|
|
Hormone replacement therapy |
|
|
|
<0.001 |
|
No |
1,825 (96.4) |
108 (90.8) |
2,676 (77.7) |
|
|
Yes |
69 (3.6) |
11 (9.2) |
767 (22.3) |
|
Table 2.Prevalence of hypertension by the stage of reproductive aging
|
Stage of reproductive aging |
Total |
Total hypertension |
Subtype of hypertensiona)
|
|
Systolic hypertension |
Diastolic hypertension |
Treated hypertension |
|
Premenopause |
1,894 |
186 (9.8) |
75 (4.0) |
100 (5.3) |
75 (4.0) |
|
Perimenopause |
119 |
30 (25.2) |
13 (10.9) |
11 (9.2) |
21 (17.7) |
|
Postmenopause |
3,443 |
955 (27.7) |
330 (9.6) |
225 (6.5) |
664 (19.3) |
REFERENCES
- 1. Mills KT, Stefanescu A, He J. The global epidemiology of hypertension. Nat Rev Nephrol 2020;16:223–37.ArticlePubMedPMC
- 2. Global Burden of Metabolic Risk Factors for Chronic Diseases Collaboration. Cardiovascular disease, chronic kidney disease, and diabetes mortality burden of cardiometabolic risk factors from 1980 to 2010: a comparative risk assessment. Lancet Diabetes Endocrinol 2014;2:634–47.ArticlePubMedPMC
- 3. World Health Organization. Global action plan for the prevention and control of noncommunicable diseases 2013-2020. Geneva, World Health Organization; 2013.
- 4. NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in blood pressure from 1975 to 2015: a pooled analysis of 1479 population-based measurement studies with 19·1 million participants. Lancet 2017;389:37–55.ArticlePubMedPMC
- 5. Kim HC, Lee H, Lee HH, Seo E, Kim E, Han J, et al. Korea hypertension fact sheet 2021: analysis of nationwide population-based data with special focus on hypertension in women. Clin Hypertens 2022;28:1. ArticlePubMedPMC
- 6. Buford TW. Hypertension and aging. Ageing Res Rev 2016;26:96–111.ArticlePubMedPMC
- 7. Lima R, Wofford M, Reckelhoff JF. Hypertension in postmenopausal women. Curr Hypertens Rep 2012;14:254–60.ArticlePubMedPMC
- 8. Barton M, Meyer MR. Postmenopausal hypertension: mechanisms and therapy. Hypertension 2009;54:11–8.ArticlePubMed
- 9. Yanes LL, Reckelhoff JF. Postmenopausal hypertension. Am J Hypertens 2011;24:740–9.ArticlePubMed
- 10. Coylewright M, Reckelhoff JF, Ouyang P. Menopause and hypertension: an age-old debate. Hypertension 2008;51:952–9.ArticlePubMed
- 11. Staessen J, Bulpitt CJ, Fagard R, Lijnen P, Amery A. The influence of menopause on blood pressure. J Hum Hypertens 1989;3:427–33.ArticlePubMed
- 12. Staessen JA, Ginocchio G, Thijs L, Fagard R. Conventional and ambulatory blood pressure and menopause in a prospective population study. J Hum Hypertens 1997;11:507–14.ArticlePubMed
- 13. Zanchetti A, Facchetti R, Cesana GC, Modena MG, Pirrelli A, Sega R, et al. Menopause-related blood pressure increase and its relationship to age and body mass index: the SIMONA epidemiological study. J Hypertens 2005;23:2269–76.ArticlePubMed
- 14. Scuteri A, Bos AJ, Brant LJ, Talbot L, Lakatta EG, Fleg JL. Hormone replacement therapy and longitudinal changes in blood pressure in postmenopausal women. Ann Intern Med 2001;135:229–38.ArticlePubMed
- 15. Luoto R, Sharrett AR, Schreiner P, Sorlie PD, Arnett D, Ephross S. Blood pressure and menopausal transition: the Atherosclerosis Risk in Communities study (1987-95). J Hypertens 2000;18:27–33.ArticlePubMed
- 16. Oh GC, Kang KS, Park CS, Sung HK, Ha KH, Kim HC, et al. Metabolic syndrome, not menopause, is a risk factor for hypertension in peri-menopausal women. Clin Hypertens 2018;24:14. ArticlePubMedPMC
- 17. van Beresteyn EC, van t Hof MA, De Waard H. Contributions of ovarian failure and aging to blood pressure in normotensive perimenopausal women: a mixed longitudinal study. Am J Epidemiol 1989;129:947–55.ArticlePubMed
- 18. Shim JS, Song BM, Lee JH, Lee SW, Park JH, Choi DP, et al. Cardiovascular and Metabolic Diseases Etiology Research Center (CMERC) cohort: study protocol and results of the first 3 years of enrollment. Epidemiol Health 2017;39:e2017016.ArticlePubMedPMC
- 19. Shim JS, Song BM, Lee JH, Lee SW, Park JH, Choi DP, et al. Cohort profile: the cardiovascular and metabolic diseases etiology research center cohort in Korea. Yonsei Med J 2019;60:804–10.ArticlePubMedPMC
- 20. Harlow SD, Gass M, Hall JE, Lobo R, Maki P, Rebar RW, et al. Executive summary of the Stages of Reproductive Aging Workshop +10: addressing the unfinished agenda of staging reproductive aging. Climacteric 2012;15:105–14.ArticlePubMedPMC
- 21. Schoenaker DA, Jackson CA, Rowlands JV, Mishra GD. Socioeconomic position, lifestyle factors and age at natural menopause: a systematic review and meta-analyses of studies across six continents. Int J Epidemiol 2014;43:1542–62.ArticlePubMedPMC
- 22. McEniery CM, Wilkinson IB, Avolio AP. Age, hypertension and arterial function. Clin Exp Pharmacol Physiol 2007;34:665–71.ArticlePubMed
- 23. Dubey RK, Oparil S, Imthurn B, Jackson EK. Sex hormones and hypertension. Cardiovasc Res 2002;53:688–708.ArticlePubMed
- 24. Rossi R, Chiurlia E, Nuzzo A, Cioni E, Origliani G, Modena MG. Flow-mediated vasodilation and the risk of developing hypertension in healthy postmenopausal women. J Am Coll Cardiol 2004;44:1636–40.ArticlePubMed
- 25. Milner TA, Contoreggi NH, Yu F, Johnson MA, Wang G, Woods C, et al. Estrogen receptor β contributes to both hypertension and hypothalamic plasticity in a mouse model of peri-menopause. J Neurosci 2021;41:5190–205.ArticlePubMedPMC
- 26. Pollow DP Jr, Romero-Aleshire MJ, Sanchez JN, Konhilas JP, Brooks HL. ANG II-induced hypertension in the VCD mouse model of menopause is prevented by estrogen replacement during perimenopause. Am J Physiol Regul Integr Comp Physiol 2015;309:R1546–52.ArticlePubMedPMC
- 27. Helvaci MR, Seyhanli M. What a high prevalence of white coat hypertension in society! Intern Med 2006;45:671–4.ArticlePubMed
- 28. Melville S, Byrd JB. Out-of-office blood pressure monitoring in 2018. JAMA 2018;320:1805–6.ArticlePubMed
- 29. Wing LM, Brown MA, Beilin LJ, Ryan P, Reid CM; ANBP2 Management Committee and Investigators. Second Autralian National Blood Pressure Study: ‘reverse white-coat hypertension’ in older hypertensives. J Hypertens 2002;20:639–44.ArticlePubMed
Citations
Citations to this article as recorded by

 , Youngrong Lee
, Youngrong Lee

 PubReader
PubReader ePub Link
ePub Link Cite
Cite