ABSTRACT
- Hypertension is a common chronic disease affecting a large section of the general population. As hypertension is usually asymptomatic, awareness, treatment and control rates are low. Drug side-effects also affect compliance. Hypotension and electrolyte abnormalities in the elderly can be severe. Therefore, prevention is better than cure. As blood pressure rises with age, prevention should be started early. As there are many genes affecting blood pressure, genetic tests are not useful. Good antenatal care and care of preterm infants can help to prevent adult cardiovascular diseases including hypertension. Childhood obesity is an important determinant of blood pressure in childhood and adolescence. This is a window of opportunity for prevention. The current American College of Cardiology/American Heart Association guideline on hypertension defines stage 1 hypertension as a systolic blood pressure of 130–139 mmHg or a diastolic blood pressure of 80–89 mmHg. Although this makes many people in the general population hypertensive, stage 1 hypertension in young adults is already associated with increased cardiovascular and mortality risk. Fortunately, hypertension at this early stage is easy to control and weight loss is easier in young males, who can get exercise from work or exercise after work. Leisure-time physical activity seems more beneficial than occupational physical activity. Cardiovascular risk assessment and promoting a healthy lifestyle in the young are likely to forestall hypertension and future cardiovascular disease. Preventing or reversing hypertension is no longer an impossible dream.
-
Keywords: Hypertension; Drug therapy; Essential hypertension; Prehypertension; Primary prevention; Secondary prevention
INTRODUCTION
- Hypertension is a chronic disease affecting a large proportion of the general population.1) About a third of adult Americans are hypertensive.2) In a large country such as China, there are a quarter of a billion adults with hypertension.3) In India, the prevalence is 33% in cities and 25% in rural areas.4) In South Korea, the prevalence is also around a third of adults.5) Hypertension is a major risk factor for coronary heart disease, strokes, heart failure and chronic kidney disease. Therefore, detecting and treating hypertension is a high priority and can reduce morbidity and mortality.
- Unfortunately, hypertension is often asymptomatic. This means that many people with hypertension are unaware of it and may not present to their doctors for diagnosis and treatment. Because of the asymptomatic nature and the fact that heart attacks and strokes occur in older adults, many younger patients with hypertension do not want to seek treatment, take regular medications and attend regular follow-ups. Therefore, the problem is more than just checking everybody's blood pressure, because there are barriers to overcome.
- A large part of the problem is that antihypertensive treatment is not very user-friendly. Most antihypertensive drugs are far from perfect. They have limited effectiveness, have adverse side-effects (Table 1)6) and need to be taken regularly. The limited efficacy of antihypertensive drugs partly stems from our lack of understanding of the pathogenesis of hypertension. In the vast majority of hypertensive patients, there is not a single cause, let alone a cause that can be removed upon treatment. In our current knowledge, blood pressure is controlled by multiple physiological systems, including the sympathetic nervous system, the reninangiotensin system and the vascular endothelium (Table 2).7) No wonder a drug that acts on a single system may not be sufficient to normalise the blood pressure in a hypertensive person. Most, if not all, antihypertensive drugs have side-effects (Table 1).6) This limits the choice of drugs and also limits dosage as higher dosages may not be tolerated. Hence, beta-blockers and thiazide diuretics are to be used at low doses. Because of ankle oedema, higher doses of the calcium channel blocker amlodipine often cannot be tolerated. Adverse drug effects also impact on compliance. Adherence to antihypertensive drug regimens is known to be poor and this has been extensively studied.8) Adverse effects of antihypertensive medications can sometimes be severe and life-threatening. Elderly hypertensive patients who are on multiple antihypertensive drugs at high doses can suffer from postural hypotension and falls, severe bradycardia as well as electrolyte abnormalities such as hyponatraemia and hypokalaemia.9)
- Prevention is better than cure. We do not have the means to cure hypertension in the great majority of patients. Can we try to prevent it? Is it preventable? The focus of this article is to discuss if hypertension is preventable, and if so, how it may be prevented.
IS HYPERTENSION PREVENTABLE?
- Although the majority of hypertensive patients have primary hypertension, meaning that no single antecedent cause can be identified, a proportion of patients have secondary hypertension (Table 3).10) In a hypertension referral clinic, these secondary causes are carefully considered and excluded. In patients presenting with hypertension at a young age,11) or in patients with difficult-to-control hypertension, it is especially important to consider and look for these secondary causes. Conn's syndrome is recognized as one of the more common causes of secondary hypertension. Among patients with resistant hypertension, spironolactone has been found to be an effective drug,12) prompting speculation that some patients with resistant hypertension may have Conn's syndrome. In recent years, there is much interest in the adrenal aldosterone-secreting adenomas.13) To diagnose these at an early stage require the 11C-metomidate positron emission tomography-computed tomography scan,14) which is not yet widely available. These adenomas can be removed laparoscopic, so these patients potentially have a form of hypertension that is curable.
- There are a small number of conditions, such as Liddle syndrome, where the patient has a single gene disorder that causes hypertension.15) However, single-gene disorders causing hypertension are rare. For the majority of patients, they may have a genetic predisposition to hypertension mediated by multiple genes. Over a hundred genes influencing blood pressure have been identified in genome-wide association studies.16) It is therefore possible to construct a genetic score that gives an indication of the genetic predisposition to hypertension. Currently, such genetic tests are costly and have no clear clinical purpose.15) For example, counselling and prenatal diagnosis are not warranted. After all, hypertension is not a life-threatening disease and is treatable. Moreover, the impact of genetics on blood pressure is small, accounting for several millimetres of mercury only.16) Intrauterine growth has a role in the pathogenesis of hypertension according to Barker's hypothesis.17) Therefore, good antenatal care has a bearing on metabolic syndrome and hypertension in later life. Work by Modi and colleagues also highlight the importance of good care of pre-term infants,18) which may help to reduce the risk of developing later in life cardiovascular diseases, including hypertension.
- Except in some rural populations, blood pressure tends to rise with age from the moment a child is born. In old age, concurrent with the rise in systolic blood pressure is a tendency for the diastolic blood pressure to decrease because of arterial stiffness.19) This results in increased pulse pressure and also the phenomenon of isolated systolic hypertension. The trajectory of blood pressure is slightly different in men and women.20) Young women have a much lower level of blood pressure than men of the same age but there is a steep rise in blood pressure around the time of menopause. As blood pressure rises with age, it means that the prevention of hypertension should be started at an early age before it becomes full-blown. This is a window of opportunity for the prevention of hypertension. Our own work suggests that childhood obesity is an important determinant of blood pressure in childhood and adolescence (Figure 1).21) Both systolic and diastolic blood pressure vary directly with body mass index or waist circumference (Figure 2).
- The relationship between blood pressure and obesity should not come as a surprise since hypertension and obesity are both components of the metabolic syndrome. The latter predicts not only the development of type 2 diabetes but also hypertension.22) In a Mendelian randomisation study, genetic variants associated with obesity were used instead of body mass index (BMI), which is affected by environmental factors.23) Those who carried genetic variants causing obesity tended to have higher blood pressure, providing strong evidence for a causal link between the two. Each 1 kg/m2 increase in BMI increased the risk of hypertension by 19%. To complete the proof that obesity causes hypertension, one can look at studies of drugs that lower bodyweight. Orlistat,24) glucagon-like peptide 1 (GLP-1) receptor agonists25) and sodium-glucose cotransporter-2 (SGLT-2) inhibitors26) all lower blood pressure along with a decrease in body weight. GLP-1 receptor agonists and SGLT-2 inhibitors, which are primarily used for the treatment of type 2 diabetes mellitus, have the additional advantage of reducing cardiovascular events.27) In case there is doubt that these drugs have a pleiotropic effect on blood pressure, a meta-analysis of bariatric surgery, which is non-pharmacological, showed a marked reduction in the risk of hypertension.28)
- There is now a global epidemic of childhood obesity.29) It is a problem of rich countries such as the USA, but also afflicts low-income countries. Poverty leads to consumption of calorie-dense foods with high glycaemic indices.30) Combating childhood obesity should be high on the agenda because if unchecked, there will be in store for the future epidemics of not only hypertension, but also type 2 diabetes and coronary heart disease.31)
EARLY-STAGE HYPERTENSION
- The 2017 American College of Cardiology/American Heart Association (ACC/AHA) guideline on the prevention, detection, evaluation and management of high blood pressure controversially redefines the thresholds for diagnosing hypertension (Table 4).32) The new definition of stage 1 hypertension includes people with a systolic blood pressure of 130–139 mmHg or a diastolic blood pressure of 80–89 mmHg. At a stroke, this increases the prevalence of hypertension in the general population33) and turns a lot of asymptomatic people in the general population into hypertensive individuals. This has been criticized for unnecessarily labelling people with a medical diagnosis,34) when most of them just need to lose weight and exercise more.
- Studies in Koreans as well as Americans suggest that stage 1 hypertension in young adults is already associated with increased cardiovascular events and mortality.35)36) Therefore, tackling stage 1 hypertension in young adults is not without reason, although the cost-effectiveness of different treatment options needs to be defined. Lifestyle treatment is likely to be cost-effective since it involves little cost to the public health system or the medical insurance.
- We have studied the characteristics of people with stage 1 hypertension in the United States National Health and Nutrition Examination Survey and found that most of them are male and obese without any history of cardiovascular disease yet (Table 5).37) Therefore, the ACC/AHA guideline recommendation of lifestyle modification for these individuals seem very appropriate.
HOW TO PREVENT HYPERTENSION?
- There is a difference between the approach to diagnosing and treating hypertension in young and old people. In young people, hypertension is often undiagnosed, but blood pressure control can usually be achieved easily. In contrast, awareness of hypertension is high in the elderly, but blood pressure is often difficult to control, resulting in a low control rate.38)
- Stage 1 hypertension should therefore be easy to control. Most of these patients do not require drug treatment.33) Exercise is easier for young males, who are more likely to have enough physical activity either at work or after work. In the retired elderly, they have fewer opportunities to have enough physical activity, and their exercise capacity might be limited by comorbidities and mobility problems. Leisure-time physical activity seems to be more beneficial than occupational physical activity.39) Therefore, current recommendations from the World Health Organisation and the American US Physical Activity Guidelines US Department of Health and Human Services (of exercising at least 150 minutes a week are highly appropriate.40)
- There are a number of new and experimental treatments for hypertension that do not involve drugs, such as renal denervation,41) splanchnic denervation,42) central iliac arteriovenous anastomosis,43) vaccine44) and gene therapy.45) Rather than curing or preventing hypertension, these technological advances are primarily aimed at patients with resistant hypertension who do not tolerate conventional drug therapy well. As most people in the general population are at risk from hypertension, especially when they live to a ripe old age, the approach to the prevention of hypertension must be safe and economical (Table 6). Lifestyle modification fits the bill very well.
CONCLUSIONS
- While detecting and adequately treating hypertension remain important goals in the management of hypertension, the prospect of preventing hypertension is very attractive.
- Cardiovascular risk assessment and promoting a healthy lifestyle in the young are likely to forestall hypertension and future cardiovascular disease.
ARTICLE INFORMATION
-
Conflict of Interest
The authors have no financial conflicts of interest.
-
Author Contributions
Writing - original draft: Cheung BM; Writing - review & editing: Tsoi MF.
Figure 1.
Relationship of systolic blood pressure with BMI and waist circumference.
BMI = body mass index; SBP = systolic blood pressure.
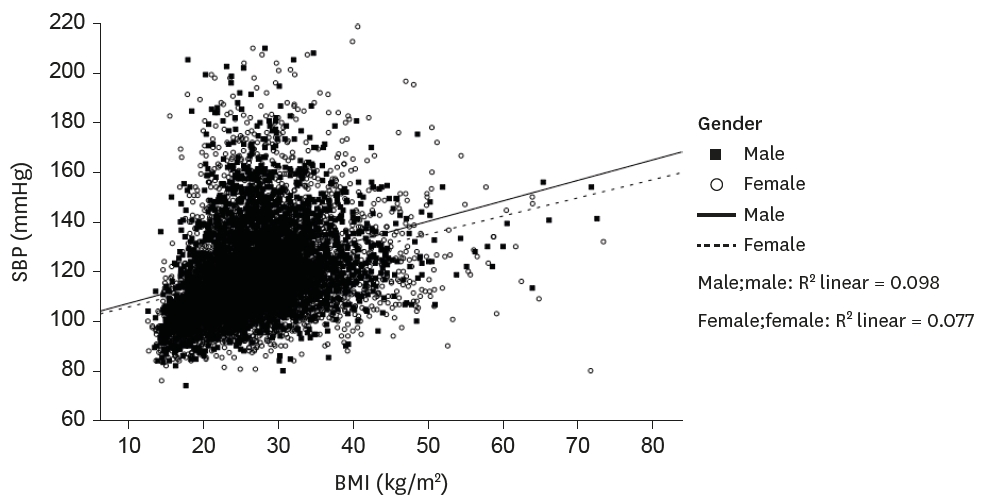
Figure 2.
Data on 3,653 boys and 3,697 girls from National Health and Nutrition Examination Survey 2007–2008 are shown.19)
The blood pressures of boys and girls are represented by filled squares and open circles, respectively. The regression lines for boys and girls are shown as full and broken lines.
SBP = systolic blood pressure.
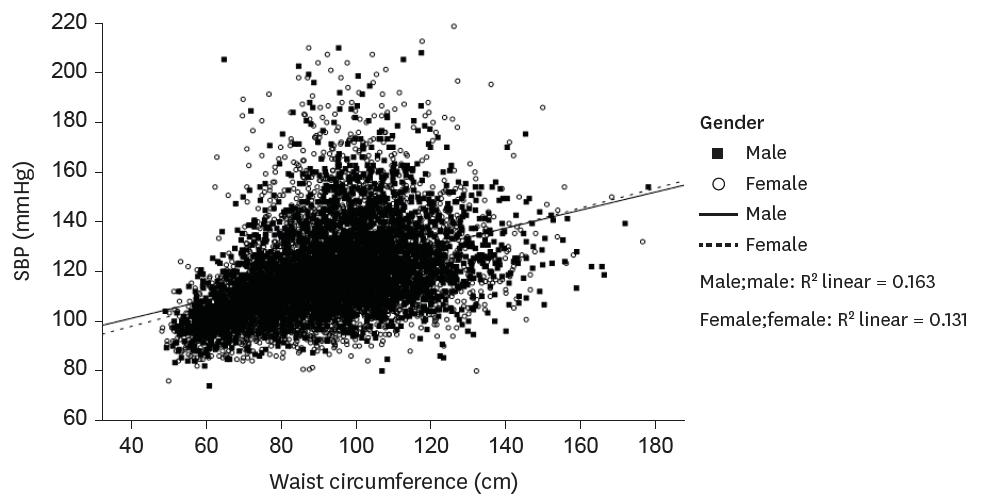
Table 1.Common adverse effects of antihypertensive drugs
|
Drug class |
Adverse effects |
|
Alpha1-adrenergic antagonist |
Postural hypotension. |
|
Angiotensin-converting enzyme inhibitors |
Cough, hyperkalemia, angio-oedema, creatinine rise. |
|
Angiotensin receptor blockers |
Hyperkalemia, creatinine rise. |
|
Beta-adrenergic blockers |
Bradycardia, fatigue, heart block, bronchospasm, intermittent claudication, cold extremities. |
|
Calcium channel blockers |
Flushing, headache, constipation, peripheral oedema. |
|
Verapamil and diltiazem are negatively chronotropic and inotropic. |
|
Diuretics, thiazide or thiazide-like |
Hypokalemia, hyponatremia, hyperuricaemia, postural hypotension. |
|
Potassium-sparing diuretics |
Hyperkalemia, gynaecomastia caused by spironolactone. |
Table 2.The major systems involved in blood pressure regulation
|
System |
Effect on blood pressure regulation |
Effect on blood pressure |
|
Sympathetic nervous system |
Catecholamine release |
↑ |
|
↑ Renal sympathetic activity |
|
|
↑ Na+ retention |
|
|
Renin-angiotensin-aldosterone system |
↑ Na+ reabsorption |
↑ |
|
↑ Aldosterone secretion |
|
|
Endothelial dysfunction |
|
|
Renal, cardiac and vascular injury |
|
|
Immune system |
↑ Macrophage infiltration |
↑ |
|
↑Na+ sensitivity |
|
|
↑ Pro-inflammatory TH1 cells |
|
|
Natriuretic peptides |
Natriuresis |
↓ |
|
Diuresis |
|
|
Vasodilation |
|
|
Endothelium |
Nitric oxide production |
↓ |
|
Vasodilation |
|
Table 3.Secondary causes of hypertension
|
Anatomical |
Coarctation of the aorta |
|
Renal |
Renal artery stenosis |
|
Polycystic kidneys |
|
Glomerulonephritis |
|
Pyelonephritis |
|
Diabetic nephropathy |
|
Other causes of renal failure |
|
Endocrine |
Hyperaldosteronism (including Conn's syndrome) |
|
Phaeochromocytoma |
|
Cushing's syndrome |
|
Acromegaly |
|
Hyperparathyroidism |
|
Respiratory |
Obstructive sleep apnoea |
|
Vasculitis |
Systemic lupus erythematosus |
|
Polyarteritis nodosa |
|
Takayasu's disease |
|
Medication |
Corticosteroid |
|
Oral contraceptive |
|
Carbenoxolone |
|
Liquorice |
|
Cyclosporin |
|
Non-steroidal anti-inflammatory drugs |
|
Venlafaxine |
|
Pseudoephedrine |
|
Substance of abuse |
Amphetamines |
|
Cocaine |
|
Ephedra |
|
Alcohol |
Table 4.Categories of blood pressure in adults in the 2017 ACC/AHA guideline
|
Blood pressure categories |
Systolic blood pressure |
|
Diastolic blood pressure |
|
Normal |
<120 mmHg |
and |
<80 mmHg |
|
Elevated |
120–129 mmHg |
and |
<80 mmHg |
|
Hypertension |
|
|
|
|
Stage 1 |
130–139 mmHg |
or |
80–89 mmHg |
|
Stage 2 |
≥140 mmHg |
or |
≥90 mmHg |
Table 5.Characteristics of adult participants with stage 1 hypertension in National Health and Nutrition Examination Survey 2015–2016
|
Characteristic |
Not on anti-hypertensive medication |
On anti-hypertensive medication |
|
Number |
558 |
396 |
|
Age (years) |
46.35±19.61 |
57.89±16.91 |
|
|
20–39 (%) |
36.62 (31.67–41.78) |
11.27 (8.29–15.14) |
|
40–59 (%) |
44.22 (37.66–50.92) |
39.74 (32.47–47.48) |
|
≥60 (%) |
19.17 (14.61–24.43) |
49.00 (41.73–56.31) |
|
Female (%) |
44.03 (40.04–48.08) |
48.59 (40.89–56.36) |
|
Systolic blood pressure (mmHg) |
128.98±9.69 |
131.78±7.96 |
|
Diastolic blood pressure (mmHg) |
77.04±17.24 |
72.60±19.51 |
|
Body mass index (kg/m2) |
30.16±7.56 |
31.58±8.36 |
|
Waist circumference (cm) |
102.39±19.37 |
106.57±24.87 |
|
Abdominal obesity US cut-offs (%)*
|
62.76 (54.64–70.38) |
73.78 (66.82–79.72) |
|
Abdominal obesity IDF cut-offs (%)†
|
79.70 (75.75–83.27) |
89.60 (83.50–93.61) |
|
History of cardiovascular disease (%) |
2.31 (1.48–3.42) |
14.45 (8.92–22.57) |
|
Diabetes mellitus (%) |
2.46 (1.31–4.18) |
3.67 (2.06–6.44) |
|
Cigarette smoking (%) |
16.82 (12.07–22.52) |
18.30 (12.99–25.15) |
Table 6.Comparison of prevention with treating only the sick
|
Prevention |
Treating the sick |
|
Scale |
Large population |
Targeted |
|
Costs |
Cost per person low |
Cost per person high |
|
Infrastructure |
Non-specialist |
Trained personnel or specialist |
|
Outcome |
Superior |
Inferior |
REFERENCES
- 1. Cheung BM, Ong KL. The challenge of managing hypertension. In: Finkel ML, editors. Public Health in the 21st Century. Vol. 1. Santa Barbara, CA, Praeger Publishing; 2011. p. 117–28.
- 2. Centers for Disease Control and Prevention: Hypertension [Internet] Atlanta, GA: Centers for Disease Control and Prevention; 2017 January Available from https://www.cdc.gov/nchs/fastats/hypertension.htmhttps://www.cdc.gov/nchs/fastats/hypertension.htm
- 3. Wang Z, Chen Z, Zhang L, Wang X, Hao G, Zhang Z, Shao L, Tian Y, Dong Y, Zheng C, Wang J, Zhu M, Weintraub WS, Gao R; China Hypertension Survey Investigators. Status of hypertension in China: results from the China hypertension survey, 2012-2015. Circulation 2018;137:2344–56.ArticlePubMed
- 4. Anchala R, Kannuri NK, Pant H, Khan H, Franco OH, Di Angelantonio E, Prabhakaran D. Hypertension in India: a systematic review and meta-analysis of prevalence, awareness, and control of hypertension. J Hypertens 2014;32:1170–7.PubMedPMC
- 5. Kim HC, Ihm SH, Kim GH, Kim JH, Kim KI, Lee HY, Lee JH, Park JM, Park S, Pyun WB, Shin J, Chae SC. 2018 Korean Society of Hypertension guidelines for the management of hypertension: part I-epidemiology of hypertension. Clin Hypertens 2019;25:16. ArticlePubMedPMC
- 6. Banach M, Aronow WS. Hypertension therapy in the older adults-do we know the answers to all the questions? The status after publication of the ACCF/AHA 2011 expert consensus document on hypertension in the elderly. J Hum Hypertens 2012;26:641–3.ArticlePubMed
- 7. Oparil S, Acelajado MC, Bakris GL, Berlowitz DR, Cífková R, Dominiczak AF, Grassi G, Jordan J, Poulter NR, Rodgers A, Whelton PK. Hypertension. Nat Rev Dis Primers 2018;4:18014. ArticlePubMedPMC
- 8. van der Laan DM, Elders PJ, Boons CC, Beckeringh JJ, Nijpels G, Hugtenburg JG. Factors associated with antihypertensive medication non-adherence: a systematic review. J Hum Hypertens 2017;31:687–94.ArticlePubMed
- 9. ACCORD Study Group, Cushman WC, Evans GW, Byington RP, Goff DC, JrGrimm RH, JrCutler JA, SimonsMorton DG, Basile JN, Corson MA, Probstfield JL, Katz L, Peterson KA, Friedewald WT, Buse JB, Bigger JT, Gerstein HC, Ismail-Beigi F. Effects of intensive blood-pressure control in type 2 diabetes mellitus. N Engl J Med 2010;362:1575–85.ArticlePubMedPMC
- 10. Sukor N. Secondary hypertension: a condition not to be missed. Postgrad Med J 2011;87:706–13.ArticlePubMed
- 11. Camelli S, Bobrie G, Postel-Vinay N, Azizi M, Plouin PF, Amar L. Prevalence of secondary hypertension in young hypertensive adults. J Hypertens 2015;33:e47.
- 12. Williams B, MacDonald TM, Morant S, Webb DJ, Sever P, McInnes G, Ford I, Cruickshank JK, Caulfield MJ, Salsbury J, Mackenzie I, Padmanabhan S, Brown MJ; British Hypertension Society's PATHWAY Studies Group. Spironolactone versus placebo, bisoprolol, and doxazosin to determine the optimal treatment for drug-resistant hypertension (PATHWAY-2): a randomised, double-blind, crossover trial. Lancet 2015;386:2059–68.ArticlePubMedPMC
- 13. Zhou J, Lam B, Neogi SG, Yeo GS, Azizan EA, Brown MJ. Transcriptome pathway analysis of pathological and physiological aldosterone-producing human tissues. Hypertension 2016;68:1424–31.ArticlePubMed
- 14. O'Shea PM; O'Donoghue D, Bashari W, Senanayake R, Joyce MB, Powlson AS, Browne D, O'Sullivan GJ, Cheow H, Mendichovszky I, Quill D, Lowery A, Lappin D, Gurnell M, Dennedy MC. 11C-Metomidate PET/CT is a useful adjunct for lateralization of primary aldosteronism in routine clinical practice. Clin Endocrinol (Oxf ) 2019;90:670–9.ArticlePubMedPDF
- 15. Burrello J, Monticone S, Buffolo F, Tetti M, Veglio F, Williams TA, Mulatero P. Is there a role for genomics in the management of hypertension? Int J Mol Sci 2017;18:1131. ArticlePubMedPMC
- 16. Warren HR, Evangelou E, Cabrera CP, Gao H, Ren M, Mifsud B, Ntalla I, Surendran P, Liu C, Cook JP, Kraja AT, Drenos F, Loh M, Verweij N, Marten J, Karaman I, Lepe MP, O'Reilly PF, Knight J, Snieder H, Kato N, He J, Tai ES, Said MA, Porteous D, Alver M, Poulter N, Farrall M, Gansevoort RT, Padmanabhan S, Mägi R, Stanton A, Connell J, Bakker SJ, Metspalu A, Shields DC, Thom S, Brown M, Sever P, Esko T, Hayward C, van der Harst P, Saleheen D, Chowdhury R, Chambers JC, Chasman DI, Chakravarti A, Newton-Cheh C, Lindgren CM, Levy D, Kooner JS, Keavney B, Tomaszewski M, Samani NJ, Howson JM, Tobin MD, Munroe PB, Ehret GB, Wain LV; International Consortium of Blood Pressure (ICBP) 1000G Analyses, BIOS Consortium; Lifelines Cohort Study, Understanding Society Scientific group, CHD Exome+ Consortium, ExomeBP Consortium; T2D-GENES Consortium, GoT2DGenes Consortium, Cohorts for Heart and Ageing Research in Genome Epidemiology (CHARGE) BP Exome Consortium, International Genomics of Blood Pressure (iGEN-BP) Consortium, UK Biobank CardioMetabolic Consortium BP working group. Genome-wide association analysis identifies novel blood pressure loci and offers biological insights into cardiovascular risk. Nat Genet 2017;49:403–15.ArticlePubMedPMC
- 17. Calkins K, Devaskar SU. Fetal origins of adult disease. Curr Probl Pediatr Adolesc Health Care 2011;41:158–76.ArticlePubMedPMC
- 18. Parkinson JR, Hyde MJ, Gale C, Santhakumaran S, Modi N. Preterm birth and the metabolic syndrome in adult life: a systematic review and meta-analysis. Pediatrics 2013;131:e1240. –63.ArticlePubMed
- 19. Safar ME. Systolic hypertension in the elderly: arterial wall mechanical properties and the reninangiotensin-aldosterone system. J Hypertens 2005;23:673–81.ArticlePubMed
- 20. Ji H, Kim A, Ebinger JE, Niiranen TJ, Claggett BL, Bairey Merz CN, Cheng S. Sex differences in blood pressure trajectories over the life course. JAMA Cardiol 2020;5:19. ArticlePubMedPMC
- 21. Cheung AJ, Cheung BM. Association of increased systolic blood pressure in children with obesity and the metabolic syndrome. J Hum Hypertens 2015;29 Suppl1:S15.
- 22. Cheung BM, Wat NM, Man YB, Tam S, Cheng CH, Leung GM, Woo J, Janus ED, Lau CP, Lam TH, Lam KS. Relationship between the metabolic syndrome and the development of hypertension in the Hong Kong Cardiovascular Risk Factor Prevalence Study-2 (CRISPS2). Am J Hypertens 2008;21:17–22.ArticlePubMed
- 23. Lee MR, Lim YH, Hong YC. Causal association of body mass index with hypertension using a Mendelian randomization design. Medicine (Baltimore) 2018;97:e11252.ArticlePubMedPMC
- 24. Sharma AM, Golay A. Effect of orlistat-induced weight loss on blood pressure and heart rate in obese patients with hypertension. J Hypertens 2002;20:1873–8.ArticlePubMed
- 25. Wang B, Zhong J, Lin H, Zhao Z, Yan Z, He H, Ni Y, Liu D, Zhu Z. Blood pressure-lowering effects of GLP-1 receptor agonists exenatide and liraglutide: a meta-analysis of clinical trials. Diabetes Obes Metab 2013;15:737–49.ArticlePubMed
- 26. Georgianos PI, Agarwal R. Ambulatory blood pressure reduction with SGLT-2 inhibitors: dose-response metaanalysis and comparative evaluation with low-dose hydrochlorothiazide. Diabetes Care 2019;42:693–700.ArticlePubMedPMC
- 27. Fei Y, Tsoi MF, Kumana CR, Cheung TT, Cheung BM. Network meta-analysis of cardiovascular outcomes in randomized controlled trials of new antidiabetic drugs. Int J Cardiol 2018;254:291–6.ArticlePubMed
- 28. Vest AR, Heneghan HM, Agarwal S, Schauer PR, Young JB. Bariatric surgery and cardiovascular outcomes: a systematic review. Heart 2012;98:1763–77.ArticlePubMed
- 29. Ng M, Fleming T, Robinson M, Thomson B, Graetz N, Margono C, Mullany EC, Biryukov S, Abbafati C, Abera SF, Abraham JP, Abu-Rmeileh NM, Achoki T, AlBuhairan FS, Alemu ZA, Alfonso R, Ali MK, Ali R, Guzman NA, Ammar W, Anwari P, Banerjee A, Barquera S, Basu S, Bennett DA, Bhutta Z, Blore J, Cabral N, Nonato IC, Chang JC, Chowdhury R, Courville KJ, Criqui MH, Cundiff DK, Dabhadkar KC, Dandona L, Davis A, Dayama A, Dharmaratne SD, Ding EL, Durrani AM, Esteghamati A, Farzadfar F, Fay DF, Feigin VL, Flaxman A, Forouzanfar MH, Goto A, Green MA, Gupta R, Hafezi-Nejad N, Hankey GJ, Harewood HC, Havmoeller R, Hay S, Hernandez L, Husseini A, Idrisov BT, Ikeda N, Islami F, Jahangir E, Jassal SK, Jee SH, Jeffreys M, Jonas JB, Kabagambe EK, Khalifa SE, Kengne AP, Khader YS, Khang YH, Kim D, Kimokoti RW, Kinge JM, Kokubo Y, Kosen S, Kwan G, Lai T, Leinsalu M, Li Y, Liang X, Liu S, Logroscino G, Lotufo PA, Lu Y, Ma J, Mainoo NK, Mensah GA, Merriman TR, Mokdad AH, Moschandreas J, Naghavi M, Naheed A, Nand D, Narayan KM, Nelson EL, Neuhouser ML, Nisar MI, Ohkubo T, Oti SO, Pedroza A, Prabhakaran D, Roy N, Sampson U, Seo H, Sepanlou SG, Shibuya K, Shiri R, Shiue I, Singh GM, Singh JA, Skirbekk V, Stapelberg NJ, Sturua L, Sykes BL, Tobias M, Tran BX, Trasande L, Toyoshima H, van de Vijver S, Vasankari TJ, Veerman JL, Velasquez-Melendez G, Vlassov VV, Vollset SE, Vos T, Wang C, Wang X, Weiderpass E, Werdecker A, Wright JL, Yang YC, Yatsuya H, Yoon J, Yoon SJ, Zhao Y, Zhou M, Zhu S, Lopez AD, Murray CJ, Gakidou E. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014;384:766–81.ArticlePubMedPMC
- 30. Chan HM, Brand-Miller JC, Holt SH, Wilson D, Rozman M, Petocz P. The glycaemic index values of Vietnamese foods. Eur J Clin Nutr 2001;55:1076–83.ArticlePubMed
- 31. Cheung BM. Hypertension: a weighty problem in children. Postgrad Med J 2017;93:647. ArticlePubMed
- 32. Whelton PK, Carey RM, Aronow WS, Casey DE Jr, Collins KJ, Dennison Himmelfarb C, DePalma SM, Gidding S, Jamerson KA, Jones DW, MacLaughlin EJ, Muntner P, Ovbiagele B, Smith SC Jr, Spencer CC, Stafford RS, Taler SJ, Thomas RJ, Williams KA Sr, Williamson JD, Wright JT Jr. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on clinical practice guidelines. Hypertension 2018;71:1269–324.ArticlePubMed
- 33. Muntner P, Carey RM, Gidding S, Jones DW, Taler SJ, Wright JT Jr, Whelton PK. Potential U.S. population impact of the 2017 ACC/AHA high blood pressure guideline. J Am Coll Cardiol 2018;71:109–18.ArticlePubMed
- 34. Miyazaki K. Overdiagnosis or not? 2017 ACC/AHA high blood pressure clinical practice guideline: Consequences of intellectual conflict of interest. J Gen Fam Med 2018;19:123–6.ArticlePubMedPMC
- 35. Son JS, Choi S, Kim K, Kim SM, Choi D, Lee G, Jeong SM, Park SY, Kim YY, Yun JM, Park SM. Association of blood pressure classification in Korean young adults according to the 2017 American College of Cardiology/American Heart Association guidelines with subsequent cardiovascular disease events. JAMA 2018;320:1783–92.ArticlePubMedPMC
- 36. Yano Y, Reis JP, Colangelo LA, Shimbo D, Viera AJ, Allen NB, Gidding SS, Bress AP, Greenland P, Muntner P, Lloyd-Jones DM. Association of blood pressure classification in young adults using the 2017 American College of Cardiology/American Heart Association Blood Pressure guideline with cardiovascular events later in life. JAMA 2018;320:1774–82.ArticlePubMedPMC
- 37. Tsoi MF, Fei Y, Cheung TT, Cheung BM. Characteristics of Americans with stage-1 hypertension: United States National Health Nutrition and Examination Survey 2011-2016. Hong Kong Med J 2018;24 Suppl 1:54.
- 38. Ong KL, Cheung BM, Man YB, Lau CP, Lam KS, Lam KS. Prevalence, awareness, treatment, and control of hypertension among United States adults 1999-2004. Hypertension 2007;49:69–75.ArticlePubMed
- 39. Or B, Tsoi MF, Cheung TT, Cheung BM. Leisure time, occupational aerobic physical activity, and mortality risk in adults of United States: National Health and Nutritional Examination Survey 2007-2016. Hong Kong Med J 2020;26 Suppl 1:13.
- 40. US Department of Health and Human Services. Physical Activity Guidelines for Americans. 2nd ed. Washington, D.C, US Department of Health and Human Services; 2018.
- 41. Bhatt DL, Kandzari DE, O'Neill WW, D'Agostino R, Flack JM, Katzen BT, Leon MB, Liu M, Mauri L, Negoita M, Cohen SA, Oparil S, Rocha-Singh K, Townsend RR, Bakris GL; SYMPLICITY HTN3 Investigators. A controlled trial of renal denervation for resistant hypertension. N Engl J Med 2014;370:1393–401.ArticlePubMed
- 42. Zhen Z, Liao SY, Zhu ZY, Sijia S, Au KW, Lai WH, Tsang A, Hai JS, Tse HF. Catheter-based splanchnic denervation for treatment of hypertensive cardiomyopathy. Hypertension 2019;74:47–55.ArticlePubMed
- 43. Lobo MD, Ott C, Sobotka PA, Saxena M, Stanton A, Cockcroft JR, Sulke N, Dolan E, van der Giet M, Hoyer J, Furniss SS, Foran JP, Witkowski A, Januszewicz A, Schoors D, Tsioufis K, Rensing BJ, Scott B, Ng GA, Schmieder RE. Central iliac arteriovenous anastomosis for uncontrolled hypertension: one-year results from the ROX CONTROL HTN trial. Hypertension 2017;70:1099–105.ArticlePubMed
- 44. Nakagami H, Morishita R. Recent advances in therapeutic vaccines to treat hypertension. Hypertension 2018;72:1031–6.ArticlePubMed
- 45. Phillips MI. Gene therapy for hypertension: the preclinical data. Hypertension 2001;38:543–8.ArticlePubMed
Citations
Citations to this article as recorded by

- The Association Between Dietary Inflammatory Index (DII) and Risk of Hypertension: A Case–Control Study
Niloofar Shoaei, Nafiseh Shokri-Mashhadi, Awat feizi, Reza Ghiasvand
High Blood Pressure & Cardiovascular Prevention.2022; 29(6): 611. CrossRef
 , Man-Fung Tsoi, PhD1
, Man-Fung Tsoi, PhD1

 PubReader
PubReader ePub Link
ePub Link Cite
Cite
