Body Weight Change and Cardiovascular Disease: Effect of Weight Gain, Weight Loss, and Weight Cycling
Article information

Abstract
Obesity is an independent risk factor for the development and progression of cardiovascular disease (CVD). Various cardiovascular outcomes are related to the association between body weight change and CVD. Metabolically healthy obese individuals could have a better prognosis in terms of cardiovascular morbidity and mortality than metabolically unhealthy obese individuals. Smoking cessation causes significant weight gain and consequent deterioration of the metabolic profile despite not impairing the cardiovascular benefits. Intentional weight loss has a consistent cardiovascular protective effect, but unintentional weight loss due to progressive catabolism and loss of muscle mass could be associated with poor cardiovascular outcomes. Obese individuals who are successful in losing weight with subsequent regain (weight cycling) could have an unfavorable cardiometabolic profile and the risk of CVD. Further studies are needed to evaluate the impact of weight changes on CVD by identifying unknown pathophysiology and to decide appropriate management and interventions for various phenotypes of weight change.
INTRODUCTION
Obesity is defined as abnormal accumulation of excess fat following the intake of energy nutrients, which exceeds the amount of used energy. The prevalence of obesity is continuously increasing, leading to a global pandemic and this prevalence has also been accelerating in Asia.1) Obesity is an independent risk factor for the development and progression of cardiovascular disease (CVD) including myocardial infarction, heart failure, stroke, thromboembolic disease, and peripheral arterial disease.2) Obesity is related to conventional risk factors of CVD such as hypertension, hyperlipidemia, and diabetes. Moreover, it increases insulin resistance and induces pro-coagulation, hypofibrinolysis, and oxidative stress through the action of inflammatory cytokines including adipokines that cause endothelial dysfunction and contribute to CVD.3)
Various cardiovascular outcomes are related to the association between body weight change and CVD. Metabolically healthy obese (MHO) individuals exhibit different body fat distribution and cardiovascular outcomes when compared with metabolically unhealthy obese (MUO) individuals.4) In addition, weight gain and consequent metabolic changes after smoking cessation (SC) are different from those associated with simple obesity.5) Unintentional loss of weight that is not due to lifestyle modifications is common among older adults and could be associated with poor cardiovascular outcomes.6) Failure to maintain a healthy weight and fluctuations in weight (commonly referred to as weight cycling) put a strain on the cardiometabolic system.7) Therefore, we aimed to review the pathophysiological mechanisms and clinical significance of weight change and its relationship with cardiovascular outcomes.
WEIGHT GAIN
Metabolically healthy vs. unhealthy obesity
Fat accumulation is heterogeneous. Subcutaneous and visceral adipose tissues differ in terms of blood flow and innervation, cell composition, and metabolic and endocrine functions.8) Unlike peripheral subcutaneous fat, visceral fat is mainly associated with the exacerbation of metabolic profiles.9)10) Regardless of the body mass index (BMI) or absolute fat volumes, a high visceral/subcutaneous adipose tissue ratio significantly worsens cardiometabolic risk and increases the possibility of subsequent CVD events.11)12) Moreover, fatty liver is associated with coronary artery calcification independent of the BMI and visceral fat.13) Thus, the risk of metabolic diseases and CVD could differ according to the phenotype of obesity, even with similar amount of weight gain. Although there is no established definition, absence of insulin resistance and metabolic disease in obese individuals is referred to as the MHO phenotype.4) In a prospective epidemiological study involving adult Caucasians, MHO individuals exhibited better fitness and better prognosis in terms of CVD mortality and morbidity than MUO individuals.14) In a meta-analysis by Kramer et al.,15) the risk of CVD was relatively lower in MHO subjects than in MUO subjects, but the risk significantly increased when compared with metabolically healthy normal-weight individuals even in the absence of metabolic abnormalities. The conversion from MHO to MUO phenotype over time has been commonly identified and is associated with an increase in the CVD risk in several studies.16)17) Therefore, MHO phenotype should not be considered a harmless condition. Further research should define MHO and evaluate its effects on CVD.
Weight gain after SC
Smoking is a modifiable risk factor for CVD and there is strong evidence suggesting the immediate benefits of SC.18) However, SC causes significant weight gain. In a meta-analysis combining 62 studies, a weight gain of approximately 4–5 kg was observed after 1 year of SC.19) Nicotine deficiency and subsequent changes in appetite and energy metabolism induced by SC lead to weight gain.5) Studies have demonstrated an increase in visceral fat and deterioration of metabolic profile characterized by elevated blood pressure and cholesterol, elevated fasting blood glucose, and insulin resistance after SC.20-22) Nevertheless, recent studies have demonstrated that weight gain and consequent worsening of metabolic profile after SC do not impair the protective benefit of SC regarding the development and prognosis of CVD.23-26)
The fear of weight gain could be associated with failure to start SC, not receiving treatment, and even relapse after SC.27)28) Some researchers have suggested that vigorous exercise combined with cognitive-behavioral therapy or medications could resolve this condition.29)30) However, there is a lack of sufficient evidence to recommend specific clinical methods for preventing weight gain after SC.31) Therefore, SC should be encouraged to lower the risk of CVD and future studies should focus on finding an appropriate intervention for weight gain and subsequent metabolic and cosmetic problems caused by SC.
WEIGHT LOSS
Intentional vs. unintentional weight loss (IWL vs. UWL)
Achieving weight loss through lifestyle modifications, bariatric surgery, or the use of drugs such as glucagon-like peptide-1 agonists in obese individuals can improve cardiometabolic conditions.32-34) IWL not only improves the metabolic profile but also improves the structure and function of the left ventricle directly or indirectly, contributing to the prevention of CVD.2) The importance of intensive lifestyle intervention through caloric restriction and exercise was strongly recognized in the Diabetes Prevention Program trial.35) Studies regarding the effectiveness of IWL in preventing CVD have demonstrated consistent cardiovascular benefits.36)37) However, some studies wherein the intention of weight loss was not identified have suggested that weight loss could be a warning sign of cardiovascular events.38)39) UWL caused by organic diseases such as malignancies, psychocognitive disorders, or unknown causes could be associated with morbidity and mortality.6) The pathophysiology of UWL is currently unknown, but it could be assumed that weight maintenance is impaired by alterations in the balance of energy intake, absorption, utilization, and loss.40) Compared to IWL, UWL was associated with older age, poorer health status, smoking, and lower BMI.41) Even after adjusting for these confounding factors, UWL was independently and significantly associated with the incidence of CVD and associated mortality.42)43) However, a meta-analysis involving 178,644 participants revealed that UWL did not show a protective effect against major adverse cardiovascular events even in overweight or obese participants.44)
Obesity paradox and sarcopenia
The concept of “obesity paradox” and CVD outcome, first introduced by Gruberg et al.,45) could be explained by the negative effect of UWL on the risk of CVD. The outcome of various CVDs including chronic heart failure showed a better “U-shaped” or “J-shaped” relationship in overweight to mildly obese individuals when compared with lean ones.46) In addition to the differences in regional fat distribution,8) the differences in molecular phenotyping of adipose tissue in this “low-risk” obesity, which is metabolically benign and protects against the risk of CVD, are in terms of following factors: secretomic profile, cell turnover and expansion, extracellular matrix fibrosis, angiogenesis, inflammation, and adipocyte browning.47) In addition, fitness is more important than “fatness” and it notably alters the relationship between obesity and CVD outcomes.48) Substantial evidence suggests that fitness is a critical component of obesity paradox and it significantly affects the major cardiovascular outcomes.14)49)50)
Sarcopenia is defined as involuntary weight loss with key characteristics of loss of muscle mass and weakening of muscle strength, resulting in poor physical performance.51) In a study involving elderly Korean individuals aged over 65 years, sarcopenia was confirmed via the loss of skeletal muscle mass on dual-energy X-ray absorptiometry in approximately 30% of the subjects and it was associated with the presence of CVD.52) Frailty (UWL with low levels of physical activity or illness) in the elderly individuals independently increases the risk of CVD and worsens the prognosis.53)54) The common factor between the obesity paradox and sarcopenia is a phenomenon that can be interpreted as a progressive catabolic state, loss of lean mass, and subsequent lack of fitness. With a progress in future research to clearly understand the pathophysiology of UWL, we should identify the intentionality and manage the causes of weight loss, bearing in mind that the risk of CVD could increase in people with loss of muscle mass and fitness, especially in elderly individuals.
Weight cycling
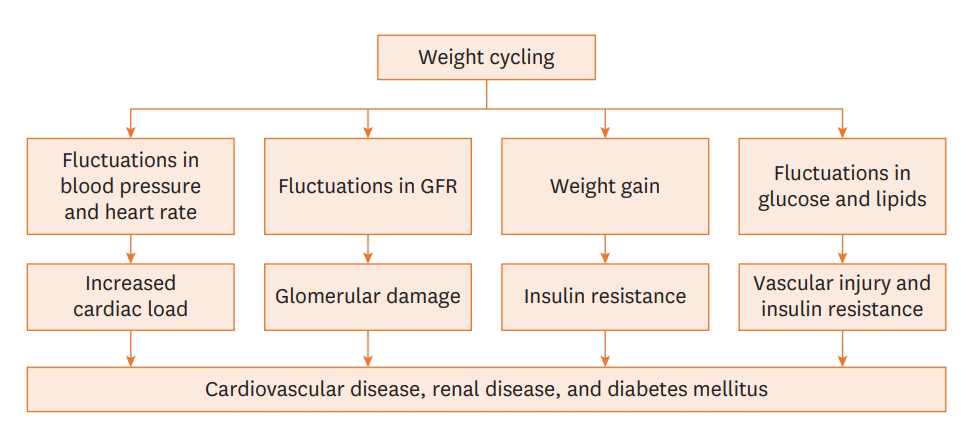
It is necessary to maintain a healthy weight in overweight or obese individuals who have achieved a healthy weight goal through intensive lifestyle intervention. However, weight regain is an important issue for those who were successful in losing weight. Weight cycling, the concept of failure to maintain a healthy weight, has a negative influence on the cardiometabolic system through increased cardiac load, glomerular damage, vascular injuries, and worsening insulin resistance (Figure 1).7) Weight cycling was related to increasing T-cell accumulation in the adipose tissue and impaired systemic glucose tolerance in an in vivo study.55) In the Look AHEAD study to understand the effect of weight regain, partial or full weight recovery was identified in the majority of the overweight and obese participants who achieved IWL of ≥3% of their initial weight.56) Furthermore, in a subsequent study by Berger et al.,57) cardiometabolic parameters that improved with weight loss deteriorated with weight regain among the participants of the Look AHEAD trial. Similar association with the deterioration of metabolic profile was consistently observed in other studies.58)59) The phenomenon of accelerated fat recovery after weight loss (catch-up fat) could explain the associations with abdominal obesity and metabolic diseases.60) The beneficial effects of cardiac structure and function achieved by weight loss are partially lost after weight is regained.61) Studies that confirmed the association of weight cycling with CVD outcomes mainly demonstrated its independent association with unfavorable CVD prevalence and prognosis.62-64) However, some researchers have argued that there was sparse evidence regarding the adverse effects of weight cycling on cardiometabolic risk and mortality.65)66)
CONCLUSION
Advancing from the past concept that emphasized only the increasing CVD risk of simple obesity and the protective effect of weight loss, a wide variety of CVD outcomes could be derived according to weight cycling as well as according to the various phenotypes of weight gain and weight loss. We suggest that it is important to evaluate not only the CVD risk with simple weight gain or BMI gain but also the causes of weight change and complementary health factors such as lean body mass and fitness. The definition of each phenotype of weight change and its categories have not been established definitively. Moreover, the pathophysiological aspects that cannot be explained by the current hypothesis remain a topic of further research. Therefore, future studies should focus on evaluating the impact of weight change on CVD by identifying unknown pathophysiology and formulating appropriate management and intervention strategies for the various phenotypes of weight change.
Notes
Conflict of Interest
The authors have no financial conflicts of interest.
Author Contributions
Supervision: Lee WY; Writing - original draft: Cho JH; Writing - review & editing: Rhee EJ, Lee WY.